GM's Cruise subsidiary has petitioned the National Highway Traffic Safety Administration (NHTSA) for permission to put the driverless Cruise Origin into commercial service. Cruise announced the filing of its petition for approval on Friday, saying the car is "a zero-emission, shared, electric vehicle that has been purposefully designed from the ground up to operate without a human driver. This means it does not rely on certain human-centered features, like a steering wheel or a sun visor, to operate safely."
Cruise said its petition, filed together with parent company GM, "demonstrates how the Origin achieves safety objectives of existing standards and helps enable future AV [autonomous vehicle] regulations." The vehicles will be manufactured at GM's "Factory ZERO" in Michigan, Cruise's announcement said. "Production is expected to begin in late 2022 in Detroit at a GM factory with vehicles delivered in 2023, Cruise said Friday," according to Reuters.
The Cruise Origin interior. (credit: Cruise)
US law allows companies to seek temporary exemptions from safety rules to deploy up to 2,500 vehicles. GM previously sought an exemption for an earlier design based on the Chevy Bolt; the NHTSA took public comment on the request for an exemption in early 2019, and GM withdrew the petition in 2020.
For The Pudding, Rebecca Monteleone and Jamie Brew (with design and code by Michelle McGhee) describe the advantages of more readable writing and how we measure readability. The best part is that they demonstrate with two versions of text. Switch paragraph-by-paragraph to see how an explanation is made more clear with simpler words and sentence structure.
HP's Pro c640 G2 enterprise Chromebook is expected to get Steam support. (credit: HP)
HP, Lenovo, Acer, and Asus are expected to be among the first companies to release gaming Chromebooks. A code change in the Chromium Gerrit suggests the vendors are working on Chrome OS devices that will support Steam.
In January 2020, Google said it would bring Steam to Chromebooks, and the plan may be starting to take shape. 9to5Google spotted a code change on Saturday showing a list of what appears to be Chromebook models that will support Steam:
When asked about the report, Acer told Ars Technica that it'd "need to defer to Google on the minimum requirements/plans for Steam on Chrome." No other laptop maker contacted got back to us in time for publication. Google has told Ars Technica in the past that a lot of experimentation happens in the Chromium Gerrit, so things can look different by the time changes hit consumers.
The Internal Revenue Service today said that selfies collected from taxpayers will be deleted and that it has deployed a new verification option as an alternative to its controversial facial recognition system. The IRS's use of the ID.me facial recognition service has been criticized by privacy and civil rights advocates as well as lawmakers from both the Democratic and Republican parties.
Two weeks ago, the IRS responded to the bipartisan backlash by saying it "will transition away from using a third-party service for facial recognition to help authenticate people creating new online accounts" and "quickly develop and bring online an additional authentication process that does not involve facial recognition." Today, the IRS announced that a new option for creating accounts without facial recognition is "now available for taxpayers."
Instead of providing a selfie, "taxpayers will have the option of verifying their identity during a live, virtual interview with agents; no biometric data—including facial recognition—will be required if taxpayers choose to authenticate their identity through a virtual interview," the IRS said.
Drivers of certain vehicles in Seattle and other parts of Western Washington are shouting at their car radios this week. Not because of any particular song or news item that’s being broadcast, but because an apparent technical glitch has caused the radios to be stuck on public radio station KUOW.
The impacted drivers appear to all be owners of Mazda vehicles from between 2014 and 2017. In some cases the in-car infotainment systems have stopped working altogether, derailing the ability to listen to the radio at all or use Bluetooth phone connections, GPS, the rear camera and more.
Behold the collision of OTA and IO(car)T. This unique situation -- limited solely to drivers in the Upper West -- presented a host of new problems and a lot of speculative answers. The radio station had absolutely no idea why this was happening. One local dealership told a customer it had something to do with 5G, which apparently meant affected Mazdas were now infected with a car-borne form of COVID, presumably necessitating plenty of expensive diagnostics and what have you.
Fortunately, the cars' manufacturer was actually able to pinpoint the cause of the malfunction -- which left some drivers staring at in-car systems stuck in a perpetual "loading…" loop. The answer arrived roughly a week after the problem presented itself. The problem -- discussed in this entertaining Reddit thread -- had nothing to do with network upgrades or an unexplained bug in Mazda software.
Instead, the public radio station had done something completely unexpected, sending affected vehicles into in-car entertainment purgatory. This is the statement Mazda gave to Geekwire.
“Between 1/24-1/31, a radio station in the Seattle area sent image files with no extension, which caused an issue on some 2014-2017 Mazda vehicles with older software,” the Mazda statement said. “Mazda North American Operations (MNAO) has distributed service alerts advising dealers of the issue.”
While it's somewhat troubling to note that Mazdas manufactured within the last eight years are running what Mazda considers to be outdated software, the good news is that it can be fixed. The bad news follows the good news: due to shipping constraints affecting goddamn everything, drivers affected by this oddity shouldn't expect to see a fix anytime soon. "Part delays" cited by Mazda could put permanent fixes months off.
On the other hand (good news!), even older models will be covered by these repairs, whether or not they're still under warranty. The company has instructed dealers to honor "goodwill requests" for free repairs of affected vehicles. Back to the bad news: the part that apparently needs to be replaced is the ominous-sounding "connectivity master unit," which indicates a whole lot of connectivity will be affected until dealers get the part in stock and start dealing with the backlog of semi-bricked Mazdas. Some users have reported in-car entertainment systems stuck in permanent loops, non-functioning GPS systems, and bricked back-up cameras.
This isn't going to go well for Mazda, considering it's the only manufacturer whose systems have been rendered useless by a misconfigured file distributed by a radio station. While this situation is certainly an outlier, there's likely a reason other in-car entertainment systems weren't similarly affected, which suggests a crucial shortcoming in the tech installed in those models -- one that could be exploited by entities far more nefarious than local public broadcasters.
A Pfizer Covid-19 vaccine vial is visible on a desk before a Senate subcommittee hearing on transporting a coronavirus vaccine on December 10, 2020, in Washington, DC. | Andrew Harnik/Getty Images
How ignoring a key side effect of Covid-19 vaccines led to one of the most pervasive vaccination myths about fertility.
The rollout of Covid-19 vaccines has laid bare some hard lessons, among them the need to fund the United States’ crumbling public health infrastructure and prioritizeequitable access to high-quality health information. But it’s also drawn attention to some long-ignored problems in the way new vaccines and other medical products are studied — including the way researchers evaluate the effects of those products on menstrual cycles.
Like most clinical trials, the 2020 Covid-19 vaccine studies didn’t collect data about menstrual variability among participants. Younger people became eligible for vaccination in early 2021, and as they did, high-profilepeople — including former Pfizer executive Michael Yeadon and feminist author Naomi Wolf —raised concerns that vaccines could negatively affect reproductive health, often in the name of women’s wellness. Menstruating people worldwide began to ask questions about whether changes in their periods portended more serious changes in their current or future ability to conceive.
Soon after,myths linking Covid-19 vaccines with infertility began spreading with surprising ferocity — facilitated, say experts, by the absence of data addressing the menstrual side effects of vaccination.
Last month, the National Institutes of Health announced publication of a study it funded on menstrual changes associated with Covid-19 vaccination, the first peer-reviewed study of its kind. Earlier availability of this data might have enabled “prebunking” of vaccine-related fertility myths, dampening their spread and impact, but by the time the NIH noted in a press release thatthe results were reassuring, the damage had already been done.
In expert circles, the immune system is known to play a role in the menstrual cycle, and events that stress the immune systemare known to cause menstrual changes. So while doctors and researchers weren’t particularly surprised to hear of minor, short-lived menstrual irregularities following vaccination, many seemed surprised by the public’sreaction to these side effects, and by the false narratives that sprang up to explain them.
Scholars of vaccine misinformation were less shocked. “A lot of misinformation has some kind of kernel of truth or is based on some kind of concern or question that is extremely valid,” said Shaydanay Urbani, who manages partnerships and programs at the misinformation research and education nonprofit First Draft. Countering that kind of information requires having good-quality data to inform people about what is true and what is not, she said.
Until recently, we did not have that data. Now, in addition to the study demonstrating a slight increase in the interval between periods, several preprint studies suggest many menstruating people likely have temporary changes in their flow after vaccination. These changes do not predict fertility problems: Multiple studies have shown that Covid-19 vaccination has no impact on the ability to conceive or safelycarry a healthy pregnancy. Conversely, Covid-19 infection poses seriousdangers to expectant parents and their pregnancies, especially for those who are unvaccinated.
Amid the many lessons we’ve learned about vaccine safety over the past two years, perhaps one of the most important is about designing future studies to avoid surges of fertility-related misinformation. “This can really be a call to action to include this type of data in future prospective clinical studies,” said Jason Wright, an OB-GYN at Columbia University and the editor-in-chief of the Obstetrics & Gynecology journal, which published the NIH study.“I hope this is the start of a bigger movement.”
Distrust in a data vacuum
It has only been 29 years since federal law required NIH-funded research to include women, and onlyrarely do studies of new vaccines or medications gather data related to menstrual changes. In 2015, the American College of Obstetricians and Gynecologists (ACOG) recommended that clinicians evaluate the menstrual cycle as the “fifth vital sign,” but assessments of menstrual outcomes as part of clinical trials are still vanishingly rare.
That’s in large part because of a concern gap between what matters to providers and what matters to patients. “Researchers just haven’t realized the importance of the menstrual cycle to women,” said Wright. While scientists may understand that the menstrual cycle is sensitive (and may vary in response) to sleep, smoking, nutrition, stress, and a host of other factors, changes in the intervals between periods and in the intensity of menstrual flow are often a mystery to individuals.
So while ACOG defines a normal interval between periods as ranging from 21 to 35 days, a two-day delay in period onset might feel wildly abnormal to someone trying to conceive or avoid pregnancy. And even if it occurred after taking a new medication or vaccine, that two-day delay mightnot register as a notable side effect to a researcher, making it unlikely to appear on the list of side effects and toxicities asked about in a study.
But failing to alert patients about a potential side effect like a change in a carefully tracked metric — for example, the timing of one’s menstrual period — can lead to fear. “If people across the board understood more, we’d be scared by a lot less,” said Brandi Shah, a Birmingham, Alabama-based family doctor who specializes in adolescent health.
Theoretically, if doctors gathered data on period changes — which clearly matter to patients — it could contribute to higher levels of public trust in medical science. But the right volume of data and the timing of its dissemination matter. “When you inundate people with good-quality information,” says Urbani, “that doesn’t necessarily mean that it’s going to change people’s behaviors or their decision-making.”
Sharing safety data about period changes early in the vaccines’ rollout might have inoculated people against later myths. While we’ve missed that opportunity, sharing this data now, especially in the visualforms and social networks where misinformation spreads fastest, can still have some corrective effect, says Urbani.
Emerging data suggests menstruating people are actually experiencing what they say they are experiencing
Three published studies have now examined vaccination-related menstrual changes in large groups of people receiving both mRNA vaccines (like Pfizer/BioNTech’s and Moderna’s) and vaccines made using virus-based technology (like Johnson & Johnson’s). This body of literature is small, and two of the published studies have not yet been peer-reviewed, meaning that they have not yet been scientifically vetted by a group of other researchers.
The studies were designed to evaluate different types of menstrual changes. While the NIH-funded study focused on changes to the length of the menstrual cycle, the other two studies also evaluated changes in flow on bleeding days and spotting between periods, and one assessed for bleeding in postmenopausal people. Of the three studies, only the peer-reviewed study included a control group of unvaccinated individuals.
The NIH-funded, peer-reviewed study looked at data people had been entering in an FDA-approved menstrual cycle tracking app since October 2020, a few months before the vaccine rollout began. (People agree that their de-identified data can be used for research when they register to use the app.)
People were prompted by the app to enter their vaccination date or confirm their unvaccinated status, and six cycles’ worth of data was assessed for each person — for vaccinated people,three cycles before and after getting their first vaccine.Ultimately, researchers analyzed data from nearly 4,000 menstruating people, about two-thirds of whom received a Covid-19 vaccine.
On average, the first period after receiving a first dose of vaccine occurred only seven-tenths of a day later than usual, indicating a minuscule but measurable lengthening of the interval between periods. No change was noted among unvaccinated people. The vast majority of participants (90 percent) received two-dose mRNA vaccines; periods were delayed by nine-tenths of a day after the second dose for those who got one.
The increase in the interval between periodswas driven mostly by the people who received both vaccine doses within a single menstrual cycle, 11 percent of whose cycles increased by eight days or more. (In comparison, only 4 percent of unvaccinated people experienced this degree of increase in their menstrual cycles.)
It makes biological sense that the subset of people vaccinated twice in one cyclewould have particularly variable intervals between periods, the investigators wrote. Two-dose vaccines are given three or four weeks apart; in order to have gotten both vaccines between periods, the first dose would’ve had to be received immediately after bleeding stopped. That phase of the cycle is particularly sensitive to illnesses and other stressors, and a catastrophic illness during this portion of the cycle (for example, severe Covid-19 infection) could permanently disrupt menstrual rhythms. However, for the smaller group experiencing eight or more days of variability, cycles returned to their usual lengths within two cycles after vaccination. The study did not identify an increase in bleeding days between or within any of the groups.
As period changes go, the cycle length is relatively easy to measure — everybody agrees on what constitutes a day. In contrast, measuring changes in flow is complicated by the variety of ways a heavier flow can surprise its owner: A heavier period can just be longer than a usual period, or it can require the use of more menstrual products for more days per period, or it can involve passing lots of clots with a period. Flow changes can also mean going from no flow — as is the experience of postmenopausal people or many of those who use hormonal IUDs for contraception or other reasons — to spotting.
Still, two studies have attempted to quantify and characterize changes in menstrual flow following vaccination. The first, with results published prior to peer review in October 2021, was designed as an emergent response to medical experts’ dismissive responses to reports of these changes, and to some patients’ conflation of short-term menstrual changes with long-term fertility harms. This study involved a survey of nearly 40,000 fully vaccinated people, including those regularly menstruating and those without regular periods (i.e., people on period-suppressing hormonal treatments and those who were post-menopausal).
More than 40 percent of the regularly menstruating respondents reported heavier bleeding after vaccination; a third of those also bled for longer. Furthermore, a surprisingly high proportion of people without regular periods had post-vaccination spotting or bleeding — 66 percent of postmenopausal people and 70 percent of those who were premenopausal — as did nearly 40 percent of people on gender-affirming hormones.
A second study, also published prior to peer review in mid-January, was prompted by a deluge of reports of post-vaccination menstrual irregularities to British and Norwegian vaccine safety assurance systems. In this study, investigators evaluated responses to a survey completed by nearly 5,700 Norwegian women ages 18 to 30 and already participating in a longer-term study observing pandemic effects on young adults. In October 2021, after having received two vaccine doses, participants were asked to recall whether they’d had a variety of menstrual symptoms during their cycles immediately preceding and following their first and second vaccine doses. Participants reported nearly twice as much heavy bleeding after their first dose of vaccination as before, and, in general, more menstrual disturbances after their second dose. There was no assessment of a return to normal menstruation.
Together, these and a handful of other, differently focused studies prove that the symptoms so many have noticed are real and relevant to people who have periods — and affirm there’s both room and reason to improve how we assess menstrual side effects of new pharmaceuticals.
The way forward
More data on post-vaccination menstrual changes is likely to emerge soon: Alison Edelman, an OB-GYN at Oregon Health and Science University who led the NIH study, said her team had gathered and was still analyzing data on flow changes following vaccination, and the European Medicines Agency recently requested an “in-depth evaluation” of available data on post-vaccination menstrual changes.
Already, a paradigm shift may be underway: Researchers designing early trials of a novel, non-Covid vaccine recently contacted Edelman about how to track menstrual changes among participants in their study. That seems like a step in the right direction. Unpleasant events are most worrisome when they come without warning, said Edelman — it’s whyairlines warn passengers about airplane turbulence, and health providers warn Covid vaccine recipients about post-vaccination fevers.
Why not menstrual changes, too?“I think it’s important that we have that information there, especially for something that people experience so frequently,” she says.
Jason Wright, the editor of the journal that published Edelman’s study, also hopes her team’s findings spur broader efforts to build assessments of menstrual side effects into future research. For now, he says, they enable doctors to provide counseling about changes in advance of vaccinations, and to reassure patients that the subject has been studied and is important to providers. “The more solid information that we can talk to patients about, I think, the better,” he says.
Techirt has long discussed how in the modern era, the things you buy aren't actually the things you buy. And the things you own aren't actually the things you own. Things you thought you owned can be downgraded, bricked, or killed off entirely without much notice. That game console with backward compatibility? It no longer has backward compatibility. That smart home hub or smart speaker at the heart of your living room setup you've enjoyed for years? It not long works. The movies and books you thought were permanently in your personal catalog? Sorry, they aren't anymore. That perfectly good two-year-old phone? It no longer gets security updates, putting you and your data at risk.
This is all bad enough when talking about smart home hubs or smart refrigerators, but it's quite another thing entirely when it comes to medical implants. IEEE Spectrum has the Cory Doctorow-esque cautionary tale of Second Sight Medical Products whose Argus optical implants were commonly installed in patients in the early aughts to help them see. Accurately heralded as immeasurably innovative at the time, these devices may soon no longer work or be supported because the company that made them is going bankrupt:
"Terry Byland is the only person to have received this kind of implant in both eyes. He got the first-generation Argus I implant, made by the company Second Sight Medical Products, in his right eye in 2004 and the subsequent Argus II implant in his left 11 years later. He helped the company test the technology, spoke to the press movingly about his experiences, and even met Stevie Wonder at a conference. “[I] went from being just a person that was doing the testing to being a spokesman,” he remembers.
Yet in 2020, Byland had to find out secondhand that the company had abandoned the technology and was on the verge of going bankrupt. While his two-implant system is still working, he doesn’t know how long that will be the case. “As long as nothing goes wrong, I’m fine,” he says. “But if something does go wrong with it, well, I’m screwed. Because there’s no way of getting it fixed."
Users went from the miracle of suddenly being able to see their first Christmas tree, to the terror of the gift being taken away from them with absolutely no recourse. Not only that, the systems that were installed create new health complications if they're left installed but stop working, and are difficult to remove -- a cost that has to be eaten by the patients. The company's patients went from having their lives revolutionized by technology to, well, the opposite:
"These three patients, and more than 350 other blind people around the world with Second Sight’s implants in their eyes, find themselves in a world in which the technology that transformed their lives is just another obsolete gadget. One technical hiccup, one broken wire, and they lose their artificial vision, possibly forever."
It's quite the cautionary tale for the entire electroceutical sector, and those who assume the cutting edge technologies that help them today will stick around for tomorrow. It's one thing for your flip phone or Betamax player to become irrelevant, it's another thing for essential health devices embedded in your skull to simply stop working because their manufacturer couldn't keep their finances in order.
Enlarge / Signage on a window of a coffee shop informs customers of their masking policy in San Francisco, California, US, on Tuesday, Feb. 15, 2022. The state's indoor mask requirement, which requires everyone to wear face coverings indoors regardless of vaccination status, expired on Wednesday. (credit: Getty | Bloomberg)
With national cases of COVID-19 dropping precipitously, the Centers for Disease Control and Prevention will soon release new guidance on how states and local governments can ease out of health restrictions, including indoor mask wearing. According to news reports citing unnamed officials, new guidance could come as early as next week.
The CDC's guidance will arrive well after several states and local governments charged ahead with plans to pull back pandemic restrictions, particularly indoor masking. The moves have left some questioning whether the CDC is, once again, struggling to keep up with the pandemic's shifting conditions.
In a press briefing last week, CDC Director Rochelle Walensky stood by the current guidance, noting that "our hospitalizations are still high, our death rates are still high." While the agency was "encouraged" by current downward trends, "we are not there yet," Dr. Walensky said of easing guidance.
The banner ad depicts the red-white-and-blue badge-shaped logo of Washington, DC’s Metropolitan Police Department. Nearby are images of two young people, as well as an encouragement for “gamers,” “foodies,” “techies,” and “influencers” to to “Join Us”—”us” being “the next generation of DC Police.” Typing in the ad’s URL or scanning its QR code will take you […]
Enlarge / Boston Medical Center Child Life Specialist Karlie Bittrich sees to a baby while in a pediatrics tent set up outside of Boston Medical Center in Boston on April 29, 2020. (credit: Getty | Boston Globe)
Despite being widely seen as mild, the omicron coronavirus variant has been brutal on children and adolescents—particularly babies and toddlers, who are still ineligible for vaccination.
According to a study published Tuesday by the Centers for Disease Control and Prevention, the peak rate of pediatric hospitalizations during the recent omicron surge was four times higher than the peak seen during delta's wave last fall. And the largest increase was seen in children ages 0 to 4, who had a peak hospitalization rate five times higher than that seen amid delta's wave.
The study authors, led by CDC emergency response team researcher Kristin Marks, were careful to note that incidental cases of COVID-19 in hospitalized children do not account for the jump in rates amid omicron. Marks and colleagues looked carefully at medical charts from hospitalized children during both the delta and omicron waves. They compared the proportions of children coming into hospitals who had COVID-19-related symptoms at admission and were marked as being admitted specifically for COVID-19. Between the two waves, they found no significant differences in those proportions.
According to a new study, the epidemic of drug-resistant pathogens is worse than researchers previously thought. | Clare Jackson/EyeEm via Getty Images
Antibiotic resistance is approaching a crisis point, and the world needs to act.
Two years ago, the CDC made a disturbing prediction: Without radical change to antibiotic use practices, drug-resistant pathogens,which at that point were estimated to cause 700,000 deaths globally every year,couldkill 10 million people per year by 2050.
A recent report published in TheLancet, however, found that the toll from antibiotic resistance is worsening even faster than expected.
Last month’s Global Research on Antimicrobial Resistance (GRAM) project report estimates that, in 2019, about 1.27 million people died directly due to antimicrobial resistance (AMR), which means cases where the patient wouldn’t have died had their infection been treatable with standard antibiotics. The total rises to 4.95 million deaths once fatalities associatedwith a drug-resistant infection, meaning that a patient died while having an identified antibiotic-resistant infection but it wasn’t clearly the immediate cause of death, are also included.
The report includes data on 23 pathogens and 88 pathogen-drug combinations in 204 countries and territories in 2019, with statistical modeling used to produce estimates for regions missing data.
The new numbers means that AMR is now among the leading causes of death worldwide, exceeding the toll of HIV/AIDS and malaria (864,000 and 643,000 deaths in 2019 respectively, according to the Lancet’s Global Burden of Disease study).HIV research attracts close to $50 billion per year in funding, but as Ramanan Laxminarayan of the Center for Disease Dynamics, Economics and Policy noted in a commentary published along with the Lancet study, “global spending on addressing AMR is probably much lower than that.”
In the last century, antibiotics have revolutionized medicine, massively cutting down mortality from common infectious diseases, while drastically improving the safety of major surgery and recovery rates from trauma. By one estimate, antibiotics have extended average human life expectancy by more than 20 years since their discovery over a century ago.
But the overuse of antibiotics, whether in human patients or in livestock, results in bacteria adapting to the drugs, leading them to become less effective over time. If the pace of resistance isn’t halted — whether through more judicious use of the drugs or through the development of new classes of antibiotics — it will likely lead to soaring deaths from common infections and surgical complications, sending us back to a world where a minor cut could potentially once again be lethal.
We can avoid this fate, but it will require coordinating a global response before it’s too late.
Antibiotic resistance, explained
Antibiotics are drugs that kill or prevent reproduction of disease-causing bacteria, without directly harming the patient’s cells. The invention of the first antibiotics changed everything, offering nothing short of a miraculous cure for severe pneumonia or wound infections that might have otherwise left patients dead.
But due to their ability to rapidly reproduce — staphylococcus, for example, can double every two hours when colonizing the human nose — and to directly exchange fragments of genetic code, bacterial pathogens evolve far more rapidly than multicellular organisms like humans. When a mutation arises that conveys resistance to an antibiotic, a large population of resistant pathogens can rapidly result, and the mutation can then be shared with other lineages of pathogen if they come into contact with each other.
Every time a patient is treated with antibiotics while a given pathogen is present, it’s a roll of the dice for a new resistance mutation to emerge. This isn’t just for human patients; the use of antibiotics for disease prevention and faster growth of livestock, which accounts for two-thirds of the total medically important antibiotics sold by weight in the US, is also a major contributor to AMR.
Resistance can develop with remarkable speed. Methicillin-resistant staphylococcus aureus, or MRSA, was first documented in 1961, just one year after the antibiotic methicillin was introduced. MRSA is actually something of a misnomer, as the pathogen is resistant to two major classes of antibiotics, penicillins and cephalosporins.
The first outbreak was documented in a Boston hospital in 1968, and for several decades most MRSA infections were seen in hospitals or other health care settings. However, by the early 2000s, community-acquired cases were rising even as hospital spread decreased. In 2019, according to the Lancet report, MRSA directly caused more than 100,000 deaths.
Resistance is the inevitable result of using antibiotics. The best we can hope for is to delay it, mitigate the consequences, and buy time for the development of new antibiotics that bacteria haven’t yet evolved resistance to.
How to resist antibiotic resistance
The Lancet study identifies three ways to slow the march of antibiotic resistance: more selective use of antibiotics, tighter infection control measures, and rapid investment in new treatments.
While the best practices for antibiotic usage in medicine are well established, they’re not always followed. Antibiotics are only effective against bacterial infections — meaning they’ll do nothing for a viral illness like influenza — and should be given only when medically necessary for an identified bacterial infection. However, a 2016 study estimates that 30 percent of the antibiotic prescriptions given in clinic visits are unnecessary.
Treatment should always start with the most narrow-spectrum antibiotic, saving for later the “big guns” — broad spectrum antibiotics, which are important to keep in reserve so they remain effective with the sickest patients, as well as newer drugs with less established resistance. Once treatment is started, it’s important for patients to finish the full course; incomplete treatment can result in a surviving population of the disease pathogen, selected for resistance, which can then infect others and spread.
Cutting down on the use of antibiotics in farming is also essential. The low-dose, prolonged regimens given to increase the rate of growth in farm animals creates ideal conditions for pathogens to evolve resistant strains, at which point these pathogens can spread to affect humans. Denmark has been a world leader here, drastically restricting non-therapeutic use of antibiotics in healthy animals solely for disease prevention and faster weight gain, but the US has yet to follow suit.
Preventing the transmission of infections within hospitals is also an essential measure to minimize the death toll from resistant bacteria; hospital-acquired infections are a major concern, with an estimated 650,000 cases annually in the US alone, and drug-resistant pathogens are much harder to treat, so maintaining isolation measures and the appropriate use of protective equipment is key.
One complication is that patients can be asymptomatic carriers without being sick, unknowingly spreading resistant bacteria. US hospitals will often test all newly admitted patients for MRSA and vancomycin-resistant enterococcus (VRE), two of the most common community-transmitted antibiotic resistant pathogens, so that carriers can be isolated from patients at risk of severe illness.
This means that reliable testing and data collection is essential to keep track of and slow the spread of resistant bacteria. That’s a particular challenge for lower-income countries; they lack the resources to test and screen patients as reliably, and they often have a shortage of and sanitation supplies. Those failings matter for rich countries as well — a globalized world means that novel resistant pathogens anywhere will present a risk elsewhere.
These control measures can buy time for pharmaceutical research companies to invest in developing new generations of antibiotics to replace existing treatments as pathogens acquire resistance to them. But progress on new antibiotics has been slow. Truly novel options — not simply tweaks on existing drugs — are what is most needed to stop drug-resistant pathogens, but the last entirely original class of antibiotics, lipopeptides, was discovered in the late 1980s.
Despite the desperate need, pharmaceutical companies are less incentivized to overcome the scientific, regulatory, and financial challenges involved in approving a new antibiotic — especially when the opportunity for profit is limited. Successfully developing an effective and nontoxic new antibiotic is a long and complex process; since 2014, more than half of the drugs being tested were discontinued before reaching the approval stage. According to a 2017 estimate, a single successful antibiotic costs $1.5 billion to bring to market, whereas the expected annual revenue per drug is less than $50 million per year.
Since the most powerful antibiotics are held in reserve as much as possible and then prescribed only as short-term treatment for acute infections, they bring in much less revenue than drugs for chronic conditions such as high blood pressure or Type 2 diabetes.
As Kevin Outterson, a Boston professor who studies antibiotic resistance, told my colleague Sigal Samuel, the problem is that “this is a product where we want to sell as little as possible. The ideal would be an amazing antibiotic that just sits on a shelf for decades, waiting for when we need it. That’s great for public health, but it’s a freaking disaster for a company.” Governments and other funders need to respond by implementing financial incentives for companies, funding academic research, or other significant changes to the current regulatory framework.
There is some good news on this front. The use of animal antibiotics decreased by 3 percent between 2019 and 2020, and the EU recently banned antibiotic administration to healthy animals. But this is far from enough.
Antimicrobial resistance has been a hidden epidemic, less visibly front and center than Covid-19, but the world cannot afford to wait to act until it reaches a crisis point.
DC’s vaccination mandate—which just went into place January 15—is ending tomorrow, February 15. Businesses with indoor venues will no longer be required to check a patron’s vaccination status, Mayor Muriel Bowser said during a press conference on Monday. Businesses can enforce their own vaccine requirements as a condition of entry, if desired. No more vaccination […]
Kamila Valieva and her coach Eteri Tutberidze. | Anne-Christine Poujoulat/AFP via Getty Images
Russian skater Kamila Valieva is a minor. The adults in her life should be held responsible.
The big question surrounding 15-year-old Kamila Valieva is whether or not she’ll be allowed to skate in the Olympic women’s individual event.
The International Testing Agency (ITA) said that Valieva, who helped the Russian women win the team event and became the first woman in history to land a quadruple jump at the Olympics, tested positive for trimetazidine, a banned heart medication that is purported to improve endurance. Russia wants her to skate, claiming a misunderstanding and perhaps Western jealousy. The ITA and the World Anti-Doping Agency (WADA) will attend a hearing on behalf of the International Olympic Committee (IOC) to appeal Russia’s decision to let her skate. The International Skating Union (ISU) will determine medals and results after the hearing, which will happen before Tuesday’s event.
Lost in the shadow of this news, perhaps, are other important questions: how a 15-year-old girl got the medication, and why she would feel like taking it was a good idea.
Valieva, along with her quad-landing teammates Alexandra Trusova and Anna Shcherbakova, all train with coach Eteri Tutberidze. Tutberidze is the single most dominant coach in women’s figure skating, as her girls — most of her skaters become champions before the age of 18 — have taken home Olympic golds and silvers, World Championships, European Championships, and international champions.
But amid all that success, none of Tutberidze’s champions have gone to multiple Olympics. They’ve retired, many citing injury, in four-year windows. Even more distressing is how there seems to be a pattern of abusive practices when it comes to diet restriction and over-training.
When the IOC, ISU, and Russia convene, they’ll decide Valieva’s future. But it would behoove them and the sport to look beyond the athlete in question and also focus on the adults in charge.
Tutberidze’s girls land jumps no other women in the world can do and are some of the most amazing skaters on the planet. But what’s the price they pay to become so?
Kamila Valieva’s coach Eteri Tutberidze has a history of injured skaters and diet restrictions
The unfortunate truth about women’s figure skating is that puberty is seen as the enemy. Smaller, leaner skaters have an advantage because of the physics involved. Lighter skaters have an easier time getting up in the air; having less mass and being narrow allows them to spin faster (think of a pencil, spinning between your fingers). Because puberty tends to add weight, height, and more fat to a woman’s body, it’s not uncommon to see it adversely affect female skaters. We’ve seen that skaters can hit more difficult jumps before they hit puberty, and then lose those jumps as their bodies change. It’s not impossible for female skaters to regain those highly difficult jumps post-puberty, but they remain the exception rather than the norm.
The downside to this, as you might expect in any elite sport, is coaches and athletes will try to physically change athletes’ bodies to keep or obtain those advantages. Hence, women’s figure skating is a sport that’s peppered with athletes who have had eating disorders like bulimia and anorexia.
Fredrik von Erichsen/picture alliance via Getty Images
Yulia Lipnitskaya performs at the Sochi Olympics.
And some of those stories have come from Eteri Tutberidze’s former students.
Back in 2014, Yulia Lipnitskaya became one of the Olympic Games’ breakout stars when she won a gold medal at 15. She was known for her spins and incredible flexibility. After Sochi 2014, she had middling results and ended her career in 2017 while suffering from a knee injury. In September of that year, she revealed to the Russian press she had been suffering from anorexia for “not just for one year, or two, or three” years and sought treatment at a rehab center in Israel. At the time, there were reports that Lipnitskaya was encouraged by Tutberidze’s team to sustain herself through “powdered nutrients” to keep the weight off.
Lipnitskaya never made it to the 2018 Olympics, where Tutberidze’s dynamic duo of Alina Zagitova and Evgenia Medvedeva shined. Zagitova and Medvedeva combined for the silver in the team event, and then went gold and silver, respectively, in the women’s singles event. At the time, Zagitova was 15 and seemed like an improved version of Lipnitskaya who could land very difficult jumps. She nabbed a gold that year.
After the Olympics, she was asked in an interview with the Russian website, Sport Express, about her growth spurt and puberty. She told them that her and her coaches’ plan to deal with the changes of puberty was to restrict her diet.
“And in terms of puberty, when you become fat — it seems to me that these are all fictions. You just need to shut your mouth and don’t eat! Or at least a little. I eat, but in small quantities,” Zagitova said.
Granted, there might be nuances lost in translation. At the time, Zagitova was 15 and may not have chosen her words wisely. But this wasn’t the first time she talked about what sounds like, at best, a very restrictive diet and, at worst, an eating disorder.
In a 2019 interview with Russian Glamour, Zagitova explained that she and team Tutberidze restricted her food intake and that she abstained from drinking water. She essentially used water as a rinse. She said:
No, I don’t like chips. Well, perhaps it’s because I don’t eat them. I like sweets — chocolate, candy. Generally, I restricted myself during the Olympic Games. I was, you can say, not drinking water at all. That is, we just rinsed our mouths and spit it all out.
In another 2019 interview, Zagitova lamented that the game had passed her by, that she was too old (at 19) to hit quads, and that if she had any hope at landing one, she’d need to first lose weight. Zagitova has since retired from the sport.
Medvedeva, who was Zagitova’s main rival, had a career punctuated with back and foot injuries. She left Tutberidze after the Olympics to train in Canada with coach Brian Orser. Orser is known for coaching champions like Yuna Kim and Yuzuru Hanyu.
While in Canada, Medvedeva opened up about how the training methods were different, and how Orser’s club did not pit her against her rivals. In a 2019 interview with the Russian site RSport, she explained how she had severely restricted her diet and was now working with a nutritionist with Orser. She seems to allude to the same calorie restriction and water weight that Zagitova references:
I understood that I should be as “dry” as possible. I weighed in Pyeongchang one and a half kilograms less than a year before the World Championships in Helsinki. It was a difficult period, but I had no other choice ... I didn’t have too many muscles then, and in this case the body retains water very much. You become heavy and “swollen.” Therefore, everything was really very tough and caused decent damage to the body. Now, fortunately, all these problems are in the past.
Medvedeva returned to Tutberidze in 2020 because of the pandemic. And in a 2021 interview with Russian media, Tutberidze said that Medvedeva gained weight and blamed Orser and Medvedeva for her poor scores. Tutberidze hasn’t been afraid of lashing out against Medvedeva and other skaters who have left her training academy. Often those skaters, like Medvedeva, return.
“So we did all we could for her under the circumstances,” Tutberidze said. In that same interview, she mentions that she trains her students 12 hours a day.
While Lipnitskaya, Zagitova, and Medvedeva are all retired now, the stories alluding to weight restriction and injury among Tutberidze’s current crop of students continue.
In a 2019 interview with Russian sports channel Sport24, Daniil Gleikhengauz, who choreographs at Tutberidze’s school, talked about Anna Shcherbakova. Shcherbakova is a favorite to medal this year. The interviewer talks about how she was amazed that Shcherbakova can eat “two shrimps” for dinner and be full.
Again, there could be nuances and humor lost in translation. The host is seemingly joking about Scherbakova’s appetite and willpower. But given Lipnitskaya’s history, Zagitova’s mentality about weight loss, and Medvedeva’s frank answers to the Russian press, the idea that Scherbakova severely restricts her diet doesn’t seem like a joke.
As former Olympic skaters, physicists, and experts explained to me earlier this month, skating is an incredibly taxing sport on the body. Hence the injuries that skaters power through to win. It’s even more terrifying to consider those injuries on the bodies of young girls who are extremely thin, severely restricting their diet, or in a scenario like Lipnitskaya’s, not eating at all.
Trusova and Scherbakova have reportedly been dealing with nagging injuries as they skate. Aliona Kostornaia, who was once seen as a lock for the Olympic team and medal threat, pulled out of the Russian Nationals this year due to an unspecified injury. And Daria Usacheva, who is one of Tutberidze’s prized pupils and Russian junior champion, appeared to suffer a very painful and serious injury this past November. Injuries are usually kept close to the vest in the Russian press.
Are skating and the media that covers it complicit?
Amid Valieva’s failed doping test and accounts of what sure seems like disordered eating and careers cut very short due to injury, it raises the question of what skating’s governing bodies are doing about this. The answer seems to be rewarding her.
In 2020, the International Skating Union awarded Tutberidze its “best coach.” And if you’ve been watching NBC’s figure skating coverage, commentator and former skater Johnny Weir has been — up until news of Valieva’s failed doping test broke — talking about spending time at her coaching facility and the splendid time he had getting to know Tutberidze and the girls. Weir posted on Instagram in November, about how thankful he was to visit the school. In hindsight, these decisions haven’t aged well.
Dimitris Isevidis/Anadolu Agency via Getty Images
Eteri Tutberidze looks on!
“If people start to look under the hood of what’s going on in Team Tutberidze, that might actually be positive for the sport because it would really shine a light on adolescent girls being abused physically, mentally, emotionally. And now pharmacologically, with these drugs,” said Dave Lease, who runs the skating analysis YouTube channel The Skating Lesson.
While he acknowledges that Tutberidze’s skaters are talented, Lease has been critical of Tutberidze on his show, specifically calling into question her training practices. He has spoken with guests about allegations of eating disorders and possible doping (prior to Valieva’s positive test). He says what’s happening at Tutberidze’s school is analogous to the abuse that happened at US Gymnastics and the Karolyis’ ranch. Saying that Tutberidze’s coaching practices are “abusive” has gotten Lease harangued in the Russian press.
“It doesn’t take a genius to realize that there’s something aberrant taking place with Tutberidze’s training methods as opposed to training methods around the rest of the world,” he said. “I don’t think that any intelligent person who follows figure skating should be surprised. The clues have been there.”
The clues Lease refers to are accounts from former skaters, but also Russian press interviews about diets, the injuries from over-training, interviews with coaches about possible doping, and Russia’s history with state-sponsored doping.
Since the news broke, former skaters like Adam Rippon and Katarina Witt have spoken out about holding Russia and the adults surrounding Valieva responsible. And in an interview with the French newspaper 20 Minutes, top ice dancing coach Romain Haguenauer said the result hadn’t surprised him. He said:
When Valieva’s name came out, I wouldn’t say people weren’t surprised, but let’s say it’s been stuff that’s been around for years. ... To see these kids between the ages of 12 and 15 doing quadruple jumps ... it’s true that there are always questions from the [jumps] specialists. I’m not one, but I know plenty of people who are and all of them have always been extremely surprised that it happened all of a sudden. Before Sochi, Russia did not shine in women’s skating. ... And then, all of a sudden, every year they bring out four new kids rocking quads.
One of the problems surrounding skating is that it goes mainstream once every four years, not unlike gymnastics. Mainstream interest peaks during the Olympics and wanes sharply after, so unless there’s something newsworthy that happens — like Valieva’s failed test — most viewers don’t follow the skaters or Tutberidze enough to know her or her skaters’ history. In Russia where these women are considered top athletes, Lease says, Tutberidze’s success outshines any criticism.
It’s also especially difficult for casual viewers to know about the controversies when you have NBC and commentators like Weir talking glowingly about the academy. For many devout skating fans, though, Tutberidze’s methods have been an open secret for years.
“I know many intelligent people who follow the sport and like to watch the sport, but maybe they aren’t completely immersed. And they prefer to watch skating and see these beautiful young skaters and be amazed and choose to look the other way,” he said. “Or they choose to not know, and not look too far into why they are so amazing.”
Radiation therapists prepare a cancer patient for treatment in the Radiation Oncology Department at Brigham and Women’s Hospital in Boston, Massachusetts, on June 10, 2020. | Craig F. Walker/The Boston Globe via Getty Images
The pandemic dramatically disrupted cancer screenings, and thousands of lives are now at stake.
Steve Serrao, chief of gastroenterology at a hospital in Moreno Valley, California, just lived through the fourth wave of Covid-19 with the omicron variant sweeping across the country. Patients in respiratory distress once again filled the hospital’s beds.
But it is another wave, one that’s starting to trickle in but is still a long way from cresting, that Serrao worries about most. He fears that the delayed diagnoses of various cancers and other chronic, life-threatening illnesses — the result of Covid-19’s disruption to routine checkups and screenings — will be the next crisis that overwhelms the US health system.
“Our next surge will be advanced chronic disease,” Serrao told me over the phone. “That’s going to be the next surge of patients who overwhelm our system. I don’t think our systems are ready.”
The Covid-19 pandemic dealt a crushing blow to the preventive services that can catch potential health problems before they become life-threatening. Screenings for several major cancers fell significantly during 2020, according to a study published in December 2021 in the journal Cancer. Colonoscopies dropped by nearly half compared to 2019, prostate biopsies by more than 25 percent. New diagnoses declined by 13 percent to 23 percent, depending on the cancer — not because there was less cancer in the world, but because less of it was being detected. The screening backlog was still growing by the end of 2020, according to this recent study, albeit at a slower rate.
“I think we are absolutely in uncharted territory,” Brian Englum, a University of Maryland surgeon who co-authored the new Cancer study, told me. “There are no examples I know of where we have seen numbers change this dramatically.”
The fear among doctors is that the pandemic’s disruption to cancer screenings and other preventive measures won’t just be a blip, although a blip would be bad enough on its own: When cancer gets diagnosed late, it’s less likely a patient’s doctors can successfully intervene, and the patient is more likely to die. Even a four-week delay in diagnosis is associated with a 6 to 13 percent higher risk of death.
But they also fear that the missed screenings will lead to a more permanent disconnect between patients and the health system. Research has found that when patients lose their primary care doctor, they tend to end up in the hospital more, with more serious health problems. People who have skipped appointments or didn’t get screenings or care may be less likely to seek it in the future, and the problems could compound.
It may take years for the consequences to become clear. Before the pandemic, some physicians questioned if the US might be conducting too many screenings. But the country is now being forced to undergo an unintended natural experiment in less screening, one with thousands of lives at stake. The collateral damage of a pandemic that has killed more than 900,000 Americans could grow even more.
“We could be years into this before we know there’s a problem,” Englum said, “and we’ve already lost a lot of people.”
“How many of these cases are out there? Nobody knows.”
Serrao described one of his patients as a Hispanic man in his 40s. When he first noticed bleeding in early 2020, the patient talked to his primary care doctor, who told him it might be hemorrhoids, Serrao said. The primary care doctor acknowledged that getting a cancer screening would be impossible on short notice because the local hospitals were so strained with Covid-19. And the patient feared he might get sick if he went to a hospital.
Ultimately, it was 18 months before the patient sought a colonoscopy. He was diagnosed with what was, by then, advanced rectal cancer, Serrao said.
If the man had come in right away, Serrao said, he might have been cancer-free after a simple polyp removal. Instead, the doctor and his team are now battling cancer that has moved into other parts of the patient’s body. His outlook is much worse than it would have been if the cancer had been caught sooner.
“How many of these cases are out there? Nobody knows,” Serrao said.
Serrao’s patient had the misfortune to notice symptoms amid the biggest disruption of medical care in US history — one that hit cancer screenings particularly hard. In April 2020, as many hospitals canceled services in order to prepare for the expected surge of Covid-19 patients, the number of colonoscopies plummeted 93 percent. Then, after a brief rebound, the late 2020 winter wave stretched hospitals and forced them to limit services. By the end of the year, there had been 133,231 fewer colonoscopies performed in 2020 compared to the 2019 baseline, 62,793 fewer chest CT scans, and 49,334 fewer fecal blood tests.
Jon Cherry/Getty Images
A pharmacy technician passes items to a nurse from a sterile area at the James Graham Brown Cancer Center in Louisville, Kentucky, on April 2, 2021.
“The drop-off in screenings has made me born again on the importance of screening,” John Marshall, chief of oncology at Georgetown University Hospital, told me. “We’re seeing more advanced diagnoses, and people presenting at a stage where they no longer can be cured.”
It will take months for the backlog to be cleared. Carrie Saia, the CEO of a community hospital in Holton, Kansas, told me that one of her facility’s gastroenterologists had been recruited by a larger Kansas City hospital to “scope from 7 in the morning to whenever at night, doing nothing but scopes.”
“They’re 1,000 people behind and backlogged right now,” Saia said. “A certain percentage out of those patients are going to have cancer growing.”
And working to clear that backlog begets a new backlog. Patients who are just now seeking a screening are finding it harder to get appointments. Marshall said he knew of patients who first experienced symptoms in September, were recommended for a screening by their doctor, but still couldn’t get an appointment as of December because there are so many patients in need of colonoscopies, MRIs, and other screening procedures.
Covid-19 led to direct rationing in overwhelmed hospitals last summer; they were unable to take patients with acute medical emergencies and couldn’t find another facility to take them. But this more subtle kind of rationing — delaying necessary services for months because the backlog has grown so large — also takes its toll, forcing doctors to make hard choices about which patients to prioritize.
“Everything is harder,” Marshall said. “We’ve had to make trade-off and priority decisions about who’s getting the treatment before the other person, decisions we would never have had to make.”
Covid-19’s disruption of US health care is likely going to deepen disparities
Serrao practices at the Riverside University Health System in San Bernardino County, about an hour and a half drive from downtown Los Angeles. Roughly two-thirds of his patients are Black, Hispanic, or Asian/Pacific Islander. Almost all of them have government insurance, either Medicare or Medicaid.
Black Americans already experience a higher incidence of and a higher mortality from colorectal cancers than white Americans. Black and Hispanic patients also tend to be diagnosed with more advanced lung cancers than their white peers, they have higher mortality from breast cancer, and they receive fewer prostate exams. At each stage, from preventive screenings to death rates, disparities already existed.
“They already have health disparities on a good day,” Serrao told me. “These last couple of years have put them back multiple years. The setback is quite profound.”
Over the course of the pandemic, Serrao’s practice struggled to make a dent in the backlog. Just as they would gain some momentum, another surge of Covid-19 would interrupt their progress.
Last January, the GI unit at his hospital was converted to a recovery area for patients receiving radiation therapy and other cancer treatments because overflow Covid-19 patients were in the space usually reserved for oncology recovery patients. As a result, he and his team couldn’t perform any screenings.
It was a necessary step — the top priority was maintaining treatment for patients already diagnosed with cancer — but it required the postponement of screenings to identify new cancer cases. The backlog got bigger.
“I’m almost certain that there are population pockets out there that have high disparities with cancer that will show up in the next year, two years, three years with more advanced cancers,” Serrao said, “and that’s because of the disruption in health care.”
Craig F. Walker/The Boston Globe via Getty Images
In response to a drop-off in screening mammography during the pandemic, Dr. Constance Lehman, shown here at Massachusetts General Hospital in Boston in July 2021, set up a program to make mammography easier by ensuring that all the follow-up testing can be done in one day.
The US will be living with the fallout of delayed cancer screenings for years
That problem may only be getting worse over time. Englum told me that one of the more troubling implications of their findings is that cancer screenings did not return to their pre-pandemic normal by the end of 2020.
It wasn’t a two- or three-month blip during the worst of the outbreak. By the end of the year, the drop in screenings looked more and more like a permanent setback. It’s the same problem we’re seeing with routine vaccinations: people who missed their shots and aren’t catching up even as we enter a new post-Covid normal.
“What our study shows is not only did we not make up for the blip, we didn’t even get back to baseline by the end of 2020,” Englum said. “We kept losing ground.”
The US health system struggled before the pandemic with managing people’s care in a timely fashion. It requires having an established relationship with a primary care doctor — which fewer and fewer Americans do — and then staying on schedule with recommended preventive screenings like colonoscopies and mammograms. As of 2018, according to a federal study, only 8 percent of Americans were receiving all the preventive services that are recommended for them.
Americans have now lived through two years when their primary care practice might have been closed, permanently or temporarily. The hospitals where they would have gotten a colonoscopy were postponing those non-emergent procedures. Some of them may have been afraid to go to the doctor or hospital, knowing that a highly transmissible virus was on the loose.
That only makes the challenge of getting people to stay on top of their health care harder. Doctors worry that people’s habits may be permanently changed by the pandemic — and not for the better.
“I am fearful that once people got out of that habit, they didn’t see an immediate problem,” Englum told me. “Then they say, ‘Well, I haven’t seen my doctor for six months or a year and nothing happened. I feel fine.’ They’re just out of the habit. They lost the routine.”
That means the health system is flying blind. Unless people get back in the habit of getting their recommended screenings, doctors will lose ground every year in identifying patients with serious conditions or at risk of developing them. That would limit their ability to get ahead of emerging health problems before they become chronic or even life-threatening.
In theory, Englum pointed out, this also could be an opportunity to learn whether the current screening guidelines are actually appropriate. If 10 years were to pass and there were no appreciable increase in cancer mortality, for example, maybe we could revise our recommendations for colonoscopies from every 10 years to every 12. The pandemic would have provided evidence such a delay doesn’t present a big risk at the population level.
That kind of reevaluation is happening across the health system. Health insurers are monitoring the outcomes for patients who delayed kidney treatment because of Covid-19. They are watching for any negative effects, but also for countervailing evidence that might indicate the missed care was actually unnecessary.
At every level, the pandemic has forced a natural experiment in what a disruption to the usual treatment plan means for patient outcomes. We are going to learn a lot, like it or not. The risk is that those lessons will come at the cost of thousands of lives.
Because the flip side of the optimistic scenario is that in 10 years’ time, we will see cancer mortality increasing as a result of delayed screenings.
“By then,” Englum said, “you’ve lost the opportunity to treat however many thousands of people.”
When most people think of the CIA (Central Intelligence Agency), they think of a foreign-facing spy agency with a long history of state sponsored coup attempts (some successful!), attempted assassinations of foreign leaders, and putting the US in the torture business. What most people don't assume about the CIA is that it's also spying on Americans. After all, we prefer our embarrassments to be foreign-facing -- something that targets (and affects) people we don't really care about and governments we have been told are irredeemable.
An entity with the power to provoke military action halfway around the world has periodically shown an unhealthy interest in domestic affairs, which are supposed to be off-limits for the nation's most morally suspect spies. The CIA (along with the FBI) routinely abuses its powers to perform backdoor searches of foreign surveillance stashes to locate US-based communications. It also has asked the FBI to do its dirty secondhand surveillance work for it in order to bypass restrictions baked into Executive Order 12333 -- an executive order issued by Ronald Reagan that significantly expanded surveillance permissions for US agencies.
Perhaps most significantly -- at least in terms of this report -- the order instructed other government agencies to be more compliant with CIA requests for information. Since its debut in December 1981, the order has been modified twice (by George W. Bush) to give the government more power.
That's the authority the CIA has been using to spy on Americans, as a recent PCLOB (Privacy and Civil Liberties Oversight Board) report shows. The PCLOB performed a "deep dive" in CIA domestic spying at the request of Senators Ron Wyden and Martin Heinrich. After its completion, the senators asked for an unclassified version of the PCLOB's report. That report has arrived. And, according to Ron Wyden's statements, it shows the CIA is utilizing EO 12333 to spy on Americans and bypass the protections (however minimal) the FISA court provides to Americans.
“FISA gets all the attention because of the periodic congressional reauthorizations and the release of DOJ, ODNI and FISA Court documents,” said Senators Wyden and Heinrich in response to the newly declassified documents. “But what these documents demonstrate is that many of the same concerns that Americans have about their privacy and civil liberties also apply to how the CIA collects and handles information under executive order and outside the FISA law. In particular, these documents reveal serious problems associated with warrantless backdoor searches of Americans, the same issue that has generated bipartisan concern in the FISA context.”
Wyden and Heinrich called for more transparency from the CIA, including what kind of records were collected and the legal framework for the collection. The PCLOB report noted problems with CIA’s handling and searching of Americans’ information under the program.
Even if the spying isn't direct, the outcome is pretty much identical to direct targeting. With EO 12333, the CIA obtains the compliance from other federal agencies envisioned by Ronald Reagan back in 1981 as his administration ran headlong into the CIA-implicating Iran-Contra scandal.
Domestic data is supposed to be "masked" if incidentally acquired by foreign-facing surveillance collections. Sometimes this simply doesn't happen. Sometimes unmasking occurs without proper permission or oversight. The FBI uses this to its advantage. So does the CIA. But the FBI handles domestic terrorism. The CIA does not. That makes the CIA's abuse possibly more egregious than the FBI's numerous violations of the same restrictions placed on domestic surveillance via foreign interception of communications by the NSA.
The PCLOB report [PDF] shows the CIA has obtained bulk financial data from other sources, possibly without proper masking of incidentally-collected US persons data. According to the CIA's response to the report, the only thing separating CIA analysts from US persons' data and communications is a pop-up box warning them that access may be illegal. This is only a warning. It does not (nor could it) prevent analysts from obtaining data they shouldn't have access to without explicit permission.
How extensive this "incidental" collection is remains to be seen. And there's a good chance no one will ever know how often this pop-up was ignored to collect data generated by US citizens and residents. Much of the report is redacted and what was shared with the PCLOB was limited to whatever the CIA felt like sharing. The oversight of programs like these is deliberately limited by the Executive Order -- one that made the assumption some things (like national security) are too important to be done properly or overseen directly.
The report does note that the CIA has internal processes to limit abuse of backdoor searches. But it also points out the CIA has read EO 12333 and its modifications to mean it can do what it wants when it wants without worrying too much about straying outside of the generous lines drawn by this Executive Order.
The limits include a requirement to use the “least intrusive collection techniques feasible within the United States or directed against United States persons abroad.” Annex A implements E.O. 12333’s “least intrusive collection technique” requirement regarding activities outside of the United States involving U.S. persons. Given that the Executive Order’s restriction only applies to activities in the United States or activities directed against U.S. persons abroad, the CIA interprets the language of Annex A to only apply to collections directed against USPs abroad. Annex A does not require [redacted] to apply the least intrusive collection technique to collections covered by this report, which are generally not directed against USPs.
There's the exploitable loop: the EO only applies to collections "directed" at US persons. Since all information is pulled from foreign-facing surveillance collections that "incidentally" collect US persons data, the resulting collection the CIA has access to is completely legal. Analysts access these collections specifically to find US persons' data, but because no agency deliberately targeted US persons, it's all above board.
This is the exploitation of foreign bulk collections to obtain information about Americans. While some may argue the damage is minimal because it only accesses information (financial records) unlikely to have an established expectation of privacy, people obviously know their financial institutions track their purchases, but that's not the same thing as people assuming the government should be able to access records -- which may contain sensitive information -- using nothing more than an Executive Order that was ostensibly written to strengthen foreign surveillance efforts.
And that's only what can be observed from this redacted release. This isn't the CIA's only attempt to hoover up info on US persons via side channels. Wyden's letter hints at FISA reforms, which likely refers to domestic phone records the NSA used to collect in bulk -- a program that was specifically targeted by Congress following the Snowden revelations. What's contained in this report is a narrow examination of one part of the CIA's exploitation of bulk collections to obtain US persons data. And if it feels this confident about its nearly unrestricted ability to perform these backdoor searches, examinations of other aspects of this program are likely to find other domestic data is ending up in the hands of CIA analysts who are supposed to be focused on foreign activities.
Enlarge / X-ray technicians take a chest X-ray of an unvaccinated COVID-19 patient on the Intensive Care Unit (ICU) floor at Hartford Hospital in Hartford, Connecticut, U.S., on Tuesday, Feb. 1, 2022. (credit: Getty | Bloomberg)
A bout of COVID-19 can take a hefty toll on the heart and blood vessels; people who recover from the infection have substantially higher risks of developing any of 20 serious cardiovascular disorders in the year following their recovery. Those disorders include heart failure, stroke, atrial fibrillation and other arrhythmias, myocarditis (inflammation of the heart), and blood clots in the lungs.
Cardiovascular risks increase with the severity of an infection—that is, people who need intensive care for COVID-19 face the highest cardiovascular risks. But, overall, the pandemic virus appears to be indiscriminate, wreaking havoc on cardiovascular systems and increasing risks in all groups of patients, from those with mild disease, to the young, to those without underlying conditions or pre-existing cardiovascular diseases.
The Food and Drug Administration, Pfizer, and BioNTech announced on Friday that they are abandoning plans to pursue the authorization of a two-dose regimen of COVID-19 vaccines for children ages 6 months to 4 years. Instead, they will again put the possibility of an authorization on hold as they await data on the efficacy of a third dose for the youngest children. That data is now expected in early April.
In a press release this afternoon, Pfizer and its partner BioNTech reported that COVID-19 cases among children enrolled in the initial two-dose trial "continue to accumulate according to the study protocol, and more data are being generated because rates of infection and illness remain high in children of this age, especially due to the recent omicron surge."
"Given that the study is advancing at a rapid pace, the companies will wait for the three-dose data as Pfizer and BioNTech continue to believe it may provide a higher level of protection in this age group," the press release continued.
Masked library patrons leave a New York Public Library in New York City on February 10. New York Gov. Kathy Hochul announced the end of the New York state indoor mask mandate effective February 10, but masks will still be required at schools, nursing homes, hospitals, and in bus and train stations. | Lokman Vural Elibol/Anadolu Agency via Getty Images
New policies unveiled this week are clashing with public health guidance.
As an exhausted nation continues to grapple with the coronavirus, Democrats are facing growing public pressure to move on to the pandemic’s next phase even as high case rates, hospitalizations, and death rates persist.
This week, several Democratic governors responded by rolling back their state’s mask mandates.
“This is a huge step back to normalcy for our kids,” New Jersey Gov. Phil Murphy said on Monday.
Such decisions come as many Americans eye a new stage of the pandemic. According to a January 20-24 Monmouth University poll, 70 percent of Americans think it’s time to accept that “Covid is here to stay and that we need to get on with our lives,” including 47 percent of Democrats, 71 percent of independents, and 89 percent of Republicans. Democrats have also weathered months of critiques from Republicans who’ve sought to frame them as the party of lockdowns, and questioned the need to mask children in schools.
Governors’ decisions this week, however, clashed with public health guidance from the Centers for Disease Control and Prevention and the White House.
“Now is not the moment” to drop mask requirements, Centers for Disease Control and Prevention chief Rochelle Walensky said in a Reuters interview this week.
The CDC still recommends masking in schools and in indoor spaces in jurisdictions with “high” or “substantial” rates of transmission. According to an NBC News analysis published on February 8, 99 percent of counties in the US would qualify by that measure.
Several of the state mask mandate changes won’t take place for weeks, and new reported cases and hospitalizations are declining nationwide. For now, it’s still unclear what the situation will be when the mandates eventually lift.
These policy changes have prompted mixed reviews from public health experts.
“I think this is a matter of political expediency, not a public health response,” John Hopkins University infectious disease epidemiologist David Celentano said of the recent moves to relax masking. “New Jersey was a ‘hot spot’ until recently; not sure they are wise to drop masking, at least for older kids.”
Amesh Adalja, a senior scholar at the Johns Hopkins Center for Health Security, noted that the decision to rescind school mask mandates in Pennsylvania has had “no major consequences.” An ABC News report has found that Covid-19 transmissions have increased in places like a Wyoming school district that recently rolled back school mask requirements, an outcome likely due to low vaccination rates among children.
The public has been divided about such policies as well. A February Axios/Ipsos poll found that just 21 percent of people support getting rid of all Covid-19 restrictions, 29 percent want to move toward opening up with “precautions,” 23 percent want leaders to mostly keep existing precautions in place, and 21 percent want more vaccine and mask requirements.
The masking rollbacks are one way Democrats are trying to navigate this confusion. And they reflect how the party is acknowledging pressure from those who want to decide for themselves how to deal with the pandemic. The new policies come despite the fact that loosening restrictions at a time with such high case rates could spur new transmissions, and could make it tougher to reinstate mandates if there were another surge. For example, in 2021, more than 20 states allowed their mask policies to expire. When the omicron variant hit this past winter, just a fraction of those states brought their mask mandates back.
“The challenge that any politician and any scientist has to grapple with is there are no 100 percent sure answers,” says Kaiser Family Foundation director of global health policy Jennifer Kates. “Do you act more cautious and risk people being angry that you’re not supporting more of a new normal or do you throw caution to the wind and risk having a setback?”
There’s still a lot of uncertainty about the pandemic
Unlike governors, the Biden administration has stopped short of indicating a shift to a new stage of the pandemic response — and instead focused on the progress made so far.
“We’ve got a way to go on that, in my view, but we’re moving,” President Joe Biden said during a January meeting with state governors, when some urged him to “move away from the pandemic.”
Part of this caution likely stems from the blowback the White House faced last year, when Biden said the country was “closer than ever to declaring our independence from a deadly virus” in a July Fourth speech, only to have delta variant cases surge in the months afterward.
“They are continuing to evaluate and there’s ongoing discussions and work happening internally,” White House press secretary Jen Psaki said at a recent press conference.
There have been major strides in the US’s pandemic response since January 2021: More than 200 million people are now fully vaccinated, the unemployment rate has gone down, and the overwhelming majority of schools are now open. Covid-19 cases are also down from the omicron peak: As of Thursday, the average number of daily cases has dipped 65 percent compared to two weeks ago, according to the New York Times tracker.
Still, according to Thursday’s data, the average number of daily cases — 205,004 — remains at 82 percent of the level seen in January 2021, and is significantly higher than the peak of 164,418 average daily cases during the Delta wave. And even though the impact of the omicron variant is waning, hospitalizations and death rates are still high as well.
As of Thursday, an average of 103,455 people have been hospitalized in the US per day, or 31 hospitalizations per day for every 100,000 people, according to the New York Times tracker. That average is comparable with the roughly 104,000 people who were hospitalized with Covid-19 at the peak of the delta wave.
In states that have recently changed policies, hospitalizations have stayed high as well. For example, New Jersey is seeing 23 hospitalizations per day per 100,000 people, Delaware is seeing 32 hospitalizations per day per 100,00 people, and New York is seeing 29 hospitalizations per day per 100,000 people.
Thursday’s national death average of 2,575 people per day is higher than it was during the delta surge as well, when there was an average of 2,000 people dying per day.
“It is troubling because it feels like this rush to ‘normal’ outweighs more preventable illness [and] death as well as is really tone-deaf to the reality that literally for millions of people across the country — there is no normal for them,” says Kristen Urquiza, the founder of Marked by Covid, a nonprofit that advocates on behalf of people who’ve lost loved ones to coronavirus.
State leaders have called for the CDC to offer more clarity about what metrics they should be looking for to determine which policies to roll back and when — but thus far, they have been left to make this decision on their own.
In that vacuum, Kates said that these decisions were likely a byproduct of both public health information and politics. “Politics is a factor here: people are tired of restrictions and governors are listening to that,” Kates told Vox.
Governors are pushing for a return to normalcy
Ahead of midterms in which Democrats are already facing headwinds, “Democrats can’t be the party of mandates,” says progressive strategist Rebecca Katz, the founder of New Deal Strategies.
Rep. Sean Patrick Maloney (D-NY), the head of the Democratic Congressional Campaign Committee, House Democrats’ campaign arm, has signaled he’s also of this school of thought. He’s among those emphasizing the need for the party to “start getting back to normal.”
Governors’ actions this week in several states including New Jersey, Delaware, and Connecticut seem to echo this viewpoint, though they’ve pushed back against suggestions that these changes were driven by political pressure.
“It’s a combination of cases, hospitalizations, positivity rates, rates of transmission all going dramatically in the right direction,” Murphy said this week.
There’s some evidence to indicate that Democrats have borne a political cost for previous Covid-19 policies, which have included school closures, though it’s far from conclusive. Masking children in schools has also become a political flashpoint in recent months.
After the Virginia gubernatorial election last year, data gathered from an 18-person focus group by Democratic strategist Brian Stryker suggested that Republicans were able to brand Democrats as the ones behind unpopular restrictive policies, including school lockdowns, and win an edge with certain voters as a result. “They felt Democrats closed their schools and didn’t feel bad about it,” Stryker’s memo reads.
A recent New Republic article by Rachel Cohen, however, noted that these policies didn’t necessarily doom Democrats, citing polling showing a majority of parents were satisfied with how their children’s schools handled the pandemic. A Hart Research Associates and Lake Research Partners survey conducted in December found that 78 percent of parents were satisfied with how their school handled the pandemic and 83 percent supported efforts the school had implemented to keep students safe. (Biden has previously been a client of Lake Research Partners.)
The January Monmouth survey saw that state mask mandates and social distancing guidance still have 52 percent of people’s support, a decline from 63 percent in September. Support for mandates was divided along party lines, with 85 percent of Democrats backing these policies, 51 percent of independents, and 24 percent of Republicans.
Still, the pushback that’s accompanied policies including school closures and mask mandates is likely a factor for Democratic leaders hoping to advance a different message in the midterms.
“The majority of the public supports mask mandates in the US and a supermajority of Democratic voters support mask mandates,” says Harvard social epidemiologist Justin Michael Feldman. “They’re not going after mainstream Democrats, they’re targeting swing voters.”
Some Democrats who recently announced changes to Covid-19 restrictions, or who have previously declined to reinstate mask mandates, are up for election this fall, including California Gov. Gavin Newsom, Illinois Gov. J.B. Pritzker, Colorado Gov. Jared Polis, Connecticut Gov. Ned Lamont, Michigan Gov. Gretchen Whitmer, Nevada Gov. Steve Sisolak, and New York Gov. Kathy Hochul.
Beyond moving away from mask mandates, Democrats are focused on a drawing a contrast with Republican leaders — including pointing to failures of GOP lawmakers to back Covid-19 relief policies and the misinformation that Republicans leaders have spread about the pandemic.
“We really are going to talk about when Republicans were in charge, they failed to crack down on the coronavirus. They unanimously opposed Democrats’ coronavirus programs that helped people get back to work, [kids] get back to school,” said DSCC spokesperson Jazmin Vargas. “Overall, it’s going to be about how we took steps to take on the coronavirus. We can effectively call out Republicans for opposing us every step of the way.”
In a study on messaging strategies, the left-leaning firm Data for Progress found “that focusing on Democratic achievements to recover from the pandemic is an effective strategy to counter Republican attacks on government interference.”
Many Republican leaders have been criticized by public health experts for lies they’ve spread about vaccines and failures to adequately promote masks and testing. But the challenge Democrats face while calling out Republicans is that Democrats are currently the party in power in the White House and Congress, and in the 16 states where Democratic governors are up for reelection.
As a result, Democrats are likely to bear any blame for continuing struggles in places where they’re in charge. That’s one reason for the growing Democratic interest in promoting an idea of “normalcy” as part of a counter to GOP critiques and public pressure — even as the pandemic is still very much happening.
So we've noted that a lot of the U.S. politician accusations that Huawei uses its network hardware to spy on Americans on behalf of the Chinese government are lacking in the evidence department. The company's been on the receiving end of a sustained U.S. government ban based on accusations that have never actually been proven publicly, levied by a country (the United States) with a long, long history of doing exactly what it accuses Huawei of doing.
To be clear, Huawei is a terrible company. It has been happy to provide IT and telecom support to the Chinese government as it wages genocide against ethnic minorities. It has also been caught helping some African governments spy on the press and political opponents. And it may very well have helped the Chinese government spy on Americans. So it's hard to feel too bad about the company.
At the same time, if you're going to levy accusations (like "Huawei clearly spies on Americans") you need to provide public evidence. And we haven't. Eighteen months of investigations found nothing. That didn't really matter much to the FCC (under Trump and Biden) or Congress, which ordered that U.S. ISPs and network operators rip out all Huawei gear and replace it to an estimated cost of $1.8 billion. Yet just a few years later, the actual cost to replace this gear has already ballooned to $5.8 billion and is likely to get higher:
"The FCC has told Congress that applications to The Secure and Trusted Communications Networks Reimbursement Program have generated requests totaling about $5.6 billion – far more than the allocated funding. The program was established to reimburse providers with 10 million or fewer customers who must remove Huawei Technologies Company and ZTE equipment."
That's quite a windfall for companies not named Huawei, don't you think?
My problem with these efforts has always been a nuanced one. I have no interest in defending a shitty global telecom gear maker with an atrocious human rights record which very well may be a proven to be a surveillance lackey for the Chinese government. Yet at the same time, domestic companies like Cisco have, for much of the last decade, leaned on unsubstantiated allegations of spying to shift market share in their favors. DC is flooded with lobbyists who can easily exploit both xenophobia and intelligence worries to their tactical advantage, then bury the need for evidence under ambiguous claims of national security:
"What happens is you get competitors who are able to gin up lawmakers who are already wound up about China,” said one Hill staffer who was not authorized to speak publicly about the matter. “What they do is pull the string and see where the top spins.”
But some experts say these concerns are exaggerated. These experts note that much of Cisco’s own technology is manufactured in China."
So my problem here isn't necessarily that Huawei doesn't deserve what's happening to it. My problem here is generally a lack of transparency in a process that's heavily dictated by lobbyists, who can hide any need for evidence behind national security claims. This creates an environment where decisions are made on a "noble and patriotic basis" that wind up being beyond common sense, reproach, and oversight. That's a nice breeding ground for fraud.
My other problem is the hypocrisy of a country that doesn't believe in limitations on spying, complaining endlessly about spying, without modifying any of its own, very similar behaviors. AT&T has been proven to be directly tethered to the NSA to the point where it's literally impossible to determine where one ends and the other begins. Yet were another country to ban AT&T from doing business there, the heads of the very same folks breathlessly concerned about surveillance ethics would explode. What makes us beyond reproach here? Our ethical track record?
And my third problem is that the almost myopic, focus on Huawei has been so massive, we've failed to take on numerous other privacy and security issues, whether that's the lack of a meaningful federal privacy law, the rampant security and privacy issues inherent in the Internet of things space (where Chinese-made hardware is rampant), or election security with anywhere close to the same level of urgency. These all are equally important issues, all exploited by Chinese intelligence, that see a small fraction of the hand-wringing and action reserved for issues like Huawei.
Again, none of this is to defend Huawei or deny it's a shitty company with dubious ethics. But the lack of transparency or skepticism creates an environment ripe for fraud and myopia by policymakers who act as if the entirety of their efforts is driven by the noblest and most patriotic of intentions. And, were I a betting man, I'd wager this whole rip and replace effort makes headlines for all the wrong reasons several years down the road.
The city of Minneapolis, Minnesota is temporarily ending the use of no-knock warrants following the killing of 22-year-old Amir Locke by Minneapolis police officers. The city's mayor, Jacob Frey, has placed a moratorium on these warrants until the policy can be reviewed by Professor Pete Kraska of Eastern Kentucky University and anti-police violence activist DeRay McKesson.
This comes as too little too late for Locke and his surviving family. The entire raid was caught on body cam and it shows Amir Locke picking up a gun (but not pointing it at officers) after he was awakened by police officers swarming into the residence.
Locke, who was not a target of the investigation, was sleeping in the downtown Minneapolis apartment of a relative when members of a Minneapolis police SWAT team burst in shortly before 7 a.m. Wednesday. Footage from one of the officers' body cameras showed police quietly unlocking the apartment door with a key before barging inside, yelling "Search warrant!" as Locke lay under a blanket on the couch. An officer kicked the couch, Locke stirred and was shot by officer Mark Hanneman within seconds as Locke held a firearm in his right hand.
Locke was shot once in the wrist and twice in the chest. He died thirteen minutes after the shooting. As you may have noticed from the preceding paragraph, Locke was not a suspected criminal. And for those who may argue simply being within reach of a firearm is justification for shooting, Locke's handgun was legal and he had a concealed carry permit. His justifiable reaction to people barging into an apartment unannounced is somehow considered less justifiable than the officers' decision to kill him.
In most cases, that's just the way it goes, which -- assuming the warrant dotted all i's and crossed all t's -- means the Second Amendment is subservient to other constitutional amendments, like the Fourth. Here's how Scott Greenfield explains this omnipresent friction in a nation where the right to bear arms is respected… but only up to a point:
The Second Amendment issue is clear. Locke had a legal gun and, upon being awoken in the night, grabbed it. He didn’t point it at anyone or put his finger on the trigger, but it was in his hand. A cop might explain that it would only take a fraction of a second for that to change, if he was inclined to point it at an officer, put his finger on the trigger and shoot. But he didn’t.
This conundrum has been noted and argued before, that if there is a fundamental personal right to keep and bear arms, and that’s what the Supreme Court informs us is our right, then the exercise of that constitutional right cannot automatically give right to police to execute you for it. The Reasonably Scared Cop Rule cannot co-exist with the Right to Keep and Bear Arms.
"Cannot co-exist." This means that, in most cases, the citizen bearing arms generally ceases to exist (along with this right) when confronted by a law enforcement officer who believes they are reasonably afraid.
There's another point to Greenfield's post that's worth reading, but one we won't discuss further in this post: the NRA's utter unwillingness to express outrage when the right to bear arms is converted to the right to remain permanently silent by police officers who have deliberately put themselves in a situation that maximizes their fears, no matter how unreasonable those fears might ultimately turn out to be.
But this is a situation that could have been avoided. A knock-and-announce warrant would have informed Locke (who was sleeping at a relative's house) that law enforcement was outside. As the owner of a legal gun and conceal/carry permit, it's highly unlikely this announcement would have resulted in Locke opening fire on officers.
It didn't have to be this way, but the Minneapolis Police Department insisted this couldn't be handled any other way.
A law enforcement source, who spoke on the condition of anonymity because of the sensitive nature of the case, said that St. Paul police filed standard applications for search warrant affidavits for three separate apartments at the Bolero Flats Apartment Homes, at 1117 S. Marquette Av., earlier this week.
But Minneapolis police demanded that, if their officers were to execute the search within its jurisdiction, St. Paul police first secure "no-knock" warrants instead. MPD would not have agreed to execute the search otherwise, according to the law enforcement source.
If it had been handled the St. Paul way, Locke might still be alive. There's no evidence here indicating deployment of a knock-and-announce warrant would have made things more dangerous for the officers. If this sort of heightened risk presented itself frequently, the St. Paul PD would respond accordingly when seeking warrants.
St. Paul police very rarely execute no-knock warrants because they are considered high-risk. St. Paul police have not served such a warrant since 2016, said department spokesman Steve Linders.
Contrast that with the Minneapolis PD, which appears to feel a majority of warrant service should be performed without niceties like knocking or announcing their presence.
A Star Tribune review of available court records found that MPD personnel have filed for, and obtained, at least 13 applications for no-knock or nighttime warrants since the start of the year — more than the 12 standard search warrants sought in that same span.
This is likely an undercount, the Star Tribune notes. Many warrants are filed under seal and are still inaccessible. But it does track with the MPD's deployment stats. According to records, the MPD carries out an average of 139 no-knock warrants a year.
This happens despite Minnesota PD policy specifically stating officers are supposed to identify themselves as police and announce their purpose (i.e., "search warrant") before entering. That rule applies even if officers have secured a no-knock warrant. If officers wish to bypass this policy that applies to no-knock warrants, they need more than a judge's permission. They also need direct permission from the Chief of Police or their designee. That's because no-knock warrants were severely restricted by police reforms passed in 2020. But it appears those reforms have done little to change the way the MPD handles its warrant business.
We'll see if the mayor's moratorium is more effective than the tepid reforms enacted following the killing of George Floyd by Officer Derek Chauvin. The undetectable change in tactics following the 2020 reforms doesn't exactly give one confidence a citywide moratorium will keep MPD officers from showing up unannounced and killing people during the ensuing confusion. It only took nine seconds for officers to end Amir Locke's life. Given what's been observed here it will apparently take several years (and several lives) before the Minneapolis PD will be willing to alter its culture and its day-to-day practices.
Enlarge / An Electrify America charging station. (credit: Electrify America)
About five years from now, a common complaint about electric vehicles—range anxiety—will be a thing of the past across much of the US.
Starting this year, the federal government will begin doling out $5 billion to states over five years to build a nationwide network of fast chargers. The plan initially focuses on the Interstate Highway System, directing states to build one charging station every 50 miles. Those stations must be capable of charging at least four EVs simultaneously at 150 kW.
Once states have completed the Interstate charging network, they’ll be able to apply for grants to fill in gaps elsewhere. The Joint Office of Energy and Transportation, a new agency formed to help the Transportation and Energy Departments administer the program, will allow case-by-case exceptions to the 50-mile requirement if, for example, no grid connection is available nearby.
Enlarge / Dr. Rochelle Walensky, director of the Centers for Disease Control and Prevention, testifies during a Senate Health, Education, Labor, and Pensions Committee hearing on Capitol Hill on January 11, 2022, in Washington, D.C. (credit: Getty | Pool)
The Centers for Disease Control and Prevention is standing by its mask guidance, despite more and more states easing recommendations as the wave of omicron cases continues to recede.
The CDC's current mask guidance says that people who are up to date on their vaccinations (i.e., vaccinated and boosted if eligible) should wear a mask in indoor public settings in any area that has substantial or high transmission. The agency defines substantial transmission as having between 50 to 99.99 new cases per 100,000 people in the past seven days. High transmission is having 100 or more new cases per 100,000 people in the past seven days.
Enlarge / Illustration of a coronal mass ejection impacting the Earth's atmosphere. These events can cause geomagnetic storms. (credit: Getty Images | Mark Garlick/Science Photo Library)
SpaceX had to ditch most of its latest batch of Starlink satellites because they were disrupted by a geomagnetic storm after being launched from the Falcon 9 rocket. Up to 40 of the 49 satellites will re-enter the atmosphere or have already done so because they were unable to reach their intended orbits.
In an update posted yesterday, SpaceX said that on February 3, the Falcon 9's second stage deployed 49 "satellites into their intended orbit, with a perigee of approximately 210 kilometers above Earth, and each satellite achieved controlled flight." SpaceX initially deploys satellites into lower altitudes than they ultimately orbit in "so that in the very rare case any satellite does not pass initial system checkouts, it will quickly be deorbited by atmospheric drag," the company said. SpaceX has licenses for altitudes of 540 km to 570 km and 335 km to 346 km.
Last week's geomagnetic storm hit a day after launch, SpaceX explained:
AT&T got a lot wrong (and still really can't admit it) with the company's $86 billion acquisition of Time Warner. There were endless layoffs, a steady dismantling of beloved brands (DC's Vertigo imprint, Mad Magazine), all for the company to lose pay TV subscribers in the end.
But the one thing the company did get right, with a little help from COVID, was its attacks on the dated, pointless, and often punitive Hollywood release window. Typically, this has involved a 90 day gap between the time a move appears in theaters and its streaming or DVD release (in France this window is even more ridiculous at three years). Generally, this is done to protect the "sanctity of the movie going experience," as if for thirty years the "sanctity of the movie going experience" hasn't involved sticky floors, over priced popcorn, big crowds and mass shootings.
During COVID, big streamers like AT&T and Comcast shifted a lot of their tentpole films (like Dune) directly to streaming, which technically saved human lives, but resulted in no limit of raised eyebrows and scorn among the "Loews at the mall is a sacred space you can't criticize" segment of Hollywood. You might recall that AMC Theaters was positively apoplectic when Comcast showed that release windows were a dated relic, declaring it would never again show a Comcast NBC Universal picture anywhere in the world if Comcast kept threatening the sacred release window (the threat lasted about a week).
WarnerMedia (in the process of being spun off by AT&T) has faced similar whining from the industry. This week the company was hit with a lawsuit (pdf) by Village Roadshow Films, which claims the company "rushed" the release of The Matrix Resurrections from 2022 to 2021 as part of an (gasp) effort to boost streaming's popularity. All through 2021, AT&T/Time Warner released films simultaneously in theaters and on streaming to boost HBO Max subscriptions. And people liked it.
Unsurprisingly, Village Roadshow Films did not, claiming the effort (dubbed "Project Popcorn") was a "clandestine plan to materially reduce box office and correlated ancillary revenue generated from tent pole films that Village Roadshow and others would be entitled to receive in exchange for driving subscription revenue for the new HBO Max service." HBO Max and AT&T telegraphed this intention, so it seems hard to argue this was somehow clandestine. The suit also accuses WarnerMedia of ignoring the fact that piracy would have hurt the overall profits to be made from the film, though, again, metrics proving clear financial harm appear lacking.
"In a statement shared with The Verge, Warner Bros. called the lawsuit “a frivolous attempt by Village Roadshow to avoid their contractual commitment to participate in the arbitration that we commenced against them last week. We have no doubt that this case will be resolved in our favor."
Again, while it's true that AT&T attacked the sacred old release window to goose streaming subscriptions, this was something that happened during an historic plague in which indoor transmission of a deadly virus could kill or disable you. It's also almost an afterthought that in the advanced home theater and mall shooting era, this is something consumers desperately wanted. For all its downsides, COVID had a strong tendency to painfully highlight shortcomings (see: broadband, the U.S. healthcare system) and dated antiquities (like release windows or a disdain for telecommuting) that no longer served us.
While there's a shrinking sect of Hollywood folks like Spielberg who still think in-person theaters and release windows are sacred and above reproach, COVID laid bare the fact that not that many people agree with them. And while that certainly disadvantaged folks financially dependent on older models (like theater owners and studios heavily vested in release windows), the reality is what it is, and a popular change was accelerated all the same.
Activists rally for voting rights outside the Supreme Court on June 23, 2021. | Drew Angerer/Getty Images
The Court’s median justice just made it much harder to stop attacks on the right to vote.
On Monday night, the Supreme Court handed down a deeply alarming decision that suggests that the Court’s Republican majority is about to cut away one of the few parts of the Voting Rights Act that it hasn’t already gutted or killed.
The immediate impact of the Court’s 5-4 decision in Merrill v. Milligan is that Alabama’s new congressional maps, which a three-judge panel that includes two Trump appointees determined to be an illegal racial gerrymander, will take effect in the 2022 election. Under those maps, only one of the state’s seven districts — or 14 percent of the US House seats — has a real shot of electing a Black lawmaker. African Americans make up about 27 percent of the state’s population.
The lower court ordered the state to draw at least two districts “in which Black voters ... have an opportunity to elect a representative of their choice.” Thus, had the lower court decision taken effect, it is likely that the racial composition of Alabama’s congressional delegation would closely match that of the state as a whole.
Monday’s order only suspends the lower court’s decision until the Court can give this case a full hearing. But the allegedly racially gerrymandered map will be in effect for the 2022 election — and it could become permanent after the Supreme Court hears and decides the full case.
One reason the Court’s order in Merrill is disturbing is that Alabama’s lawyers offered an exceptionally weak legal argument when they asked the justices to block this lower court order. Their argument could potentially neutralize an important safeguard against racist gerrymanders.The Voting Rights Act provides fairly robust protections against racial gerrymanders — legislative maps that target voters of a particular race — but Alabama asked the Supreme Court to impose a new burden on plaintiffs challenging racial gerrymanders that may be impossible to overcome.
Justice Brett Kavanaugh wrote a separate concurring opinion that would impose a novel new restriction on all voting rights cases. More on the specific convoluted restriction later. But in creating his new restriction, Kavanaugh relied heavily on Purcell v. Gonzalez (2006), a decision which held that courts should be reluctant to change a state’s election rules as an election draws close. “Federal courts ordinarily should not enjoin a state’s election laws in the period close to an election,” Kavanaugh wrote.
There’s still a fairly obvious problem with Kavanaugh’s opinion. Alabama will not elect its new slate of US House members until November. It’s now February — nine months before the date of the general election and more than three months before the state’s next primary election. The state simply is not in a “period close to an election,” unless we count the entirety of 2022, and therefore the entirety of any year in which an election is held, as “close to an election.”
Technically, Kavanaugh’s opinion is not a binding precedent. It was joined only by Justice Samuel Alito, not by a majority of the Court. But Kavanaugh is also the median vote on this Republican-dominated Supreme Court — in politically charged cases, there are normally four justices to Kavanaugh’s left, and four to his right. That means that his words carry an unusual amount of weight, since it is unlikely that a litigant will find five justices willing to contradict him.
The bottom line is that Merrill — even in its temporary form — is a disaster for voting rights. It suggests that the Court is going to escalate its assault on the Voting Rights Act — and on voting rights more broadly. And it suggests that even exceedingly weak legal arguments offered by red states have a very good shot of prevailing in this Supreme Court.
Chip Somodevilla/Getty Images
Hundreds of protesters rally outside the Hart Senate Office Building in Washington, DC, on August 2, 2021.
Kavanaugh would strip the federal judiciary of much of its power to protect voting rights
When Purcell was handed down in 2006, it largely went unnoticed by anyone who isn’t an election lawyer. Purcell warned that “court orders affecting elections ... can themselves result in voter confusion and consequent incentive to remain away from the polls,” and that this risk increases “as an election draws closer.”
No justice dissented in Purcell, and its warning about court orders that disrupt elections is best read as a note of caution. Purcell was correct that voters might be confused about how to vote if, say, a court were to order a bunch of polling precincts to be relocated on the eve of an election. So the Court asked judges to be careful about such last-minute orders without actually forbidding them in especially compelling cases.
But as the Court grew more conservative, it seemed to treat Purcell less as a reason for caution and more like a firm command. The Court’s Republicans relied on Purcell, for example, to halt lower court orders that would have made it easier to cast a ballot at the height of the pandemic.
Kavanaugh’s opinion in Merrill would expand Purcell even further if adopted. Alabama enacted its congressional maps on November 4, 2021, and the lower court handed down its decision striking down those maps on January 24, 2022 — well more than nine months before the general election.
Moreover, as Justice Elena Kagan notes in a dissenting opinion, the lower court heard “over seven days of testimony” and received “more than 1,000 pages of briefing.” The lower court opinion striking Alabama’s maps is 225 pages long. It’s unclear how these three judges could have moved any faster and still worked through the complicated factual questions in Merrill in a careful and judicious manner.
So one upshot of Kavanaugh’s opinion is that the Purcell window — the period that counts as “close to an election” — should extend for more than nine months. That’s such a long period of time when courts cannot hand down “orders affecting elections” that it would be helpful if Kavanaugh informed us when, exactly, a judge is allowed to hand down an order impacting a state’s election laws.
In fairness, Kavanaugh does write that there are some cases when Purcell should not apply, even if an election is about to happen. But he writes that lower courts are bound by Purcell unless “the underlying merits” of a case “are entirely clearcut in favor of the plaintiff.”
Chip Somodevilla/Getty Images
Then-Supreme Court nominee Judge Brett Kavanaugh holds up a small copy of the U.S. Constitution while answering questions before the Senate Judiciary Committee during the second day of his Supreme Court confirmation hearing on Capitol Hill on September 5, 2018.
Here as well, his opinion goes off the rails. As Chief Justice John Roberts writes in dissent, “the District Court properly applied existing law in an extensive opinion with no apparent errors for our correction.” (Roberts isn’t exactly known as a champion of voting rights. The fact that he accuses his Court of going too far in a voting rights case is itself remarkable.)
The underlying merits of Merrill are clear under existing law. Kavanaugh’s suggestion that the proper outcome is unclear only makes sense if you presume that longstanding Supreme Court precedents should be tossed out.
Thus, the upshot of Kavanaugh’s opinion appears to be two-fold. First, Kavanaugh would extend the Purcell window so that it apparently encompasses the entire election year. And, second, he would forbid judges from ruling in favor of voting rights plaintiffs during this window, even if those judges faithfully apply existing law, if Kavanaugh personally believes that this law should be changed.
How else should we understand Kavanaugh’s implication that this relatively straightforward case is not clear-cut?
Alabama seeks an unprecedented new restriction on the Voting Rights Act
The Court’s precedents governing racial gerrymandering are, admittedly, quite messy.
When a plaintiff alleges that a state’s legislative maps violate the Voting Rights Act — like the plaintiffs in the Alabama case are alleging — courts typically must apply the multi-step analysis that the Court laid out in Thornburg v. Gingles (1986). The last step of this analysis requires judges to weigh at least nine different factors before striking down a state’s legislative map.
In Merrill, however, Alabama did not attack any of the more confusing parts of the Gingles framework. Indeed, it made the baffling decision to attack what may be the most straightforward part of this framework.
Under Cooper v. Harris(2017), a fairly recent decision applying Gingles, a plaintiff who believes that a state should have an additional district where a particular minority group is in the majority must show that this group is “sufficiently large and geographically compact” that it is actually possible to draw a new district where they “constitute a majority.”
The purpose of this requirement, as Justice Kagan explains in her Merrill dissent, is to require voting rights plaintiffs to prove from the outset that “what they are asking for is possible.” There’s no point allowing a lawsuit to move forward if a court cannot actually give the plaintiffs what they seek.
In any event, the plaintiffs in Merrill cleared this very low bar. One set of plaintiffs, for example, hired a mathematician to produce four sample maps that feature compact districts, and that include two Black-majority districts.
US District Court for the Northern District of Alabama
Four maps produced by mathematician Moon Duchin show how Black-majority congressional districts could be drawn in Alabama.
Alabama, however, asked the Supreme Court to impose a new restriction. According to the state, the Merrill plaintiffs erred because, in order to produce these sample maps, the plaintiffs had to “prioritize race first and consider other race-neutral factors second” — something the state claims is not allowed.
But this objection makes no sense. Again, Gingles and Cooper require a plaintiff who alleges that a state should have two Black-majority districts to first produce sample maps with two Black-majority districts. How is it even possible to complete that task without paying close attention to race?
As Kagan writes, “at no time has this Court held that plaintiffs must answer the race-infused question of the first Gingles condition without any awareness of race.”
Kagan does acknowledge one other possibility: “Plaintiffs can now use technology to generate millions of possible plans, without any attention to race,” she writes, and some of these randomly drawn maps would presumably contain two Black-majority districts.
But really, what’s the point of imposing such a burden on voting rights plaintiffs? Asking these plaintiffs to produce millions of random maps and then hunt through them to find some that include two Black-majority districts is a bit like asking Vox Media to fire its writers and replace them with a million monkeys banging away at a million typewriters.
Eventually, those monkeys would produce an analysis of the Supreme Court’s decisions that is just as trenchant as anything I could write — but only after churning out countless pages of gibberish.
In any event, Kavanaugh appears to believe that it is not “entirely clearcut” whether the Voting Rights Act requires the Merrill plaintiffs to use the monkeys-banging-on-typewriters method to produce sample maps.
While the Court figures that out, a total of five justices agreed to halt the lower court’s order and allow a racial gerrymandered map to be used in Alabama in 2022.
Enlarge / The Pixel 3 XL and Pixel 3. (credit: Ron Amadeo)
The February Android security patch is live, marking both the first on-time patch for the Pixel 6 and the last patch ever for the Pixel 3.
The Pixel 3 launched in October 2018 to lukewarm reviews, thanks to a giant camera notch on the XL model and a worrying dearth of RAM across the lineup. Google only offers three years of major OS updates (even on the Pixel 6), so the phone's last regular update was the Android 12 launch in October 2021. Pushing one of the biggest Android launches ever as the final update is a little scary (there are bound to be some bugs), so Google promised one last wrap-up update before it said goodbye to the Pixel 3. The device ended up with two more updates: one in January to patch that wild 911 bug and this final update. Google hasn't posted any release notes for the last Pixel 3 update, but the February update should cover all the security issues up to today, and from now on, you're out of date.
The Pixel 6's update plan is promoted by Google as "five years of Android security updates," but that still includes only three years of major Android version updates. The Pixel 6 will be obsolete in October 2024, but it will continue to get security updates until October 2026. We've long seen Android companies blame SoC vendors for the short support times compared to the iPhone's six years of updates, but with the Google Tensor, Google is its own SoC vendor now, so it could support the Pixel 6 for longer if it wanted.
Hyundai and Kia have issued a recall for nearly 485,000 SUVs (and a handful of sedans) due to the risk of engine bay fires, warning owners to park the vehicles outside until the repair work has been completed.
The problem affects 126,747 Kias—certain K900 sedans from model years 2016–2018 and all Sportage SUVs from model years 2014–2016.
Hyundai has a bigger task, as it's recalling 357,830 vehicles split between the Santa Fe (model years 2016–2018, not equipped with smart cruise control), the Santa Fe Sport (model years 2017-2018, not equipped with smart cruise control), the Santa Fe XL (model-year 2019, not equipped with smart cruise control), and the Tucson (model years 2014–2015).
We've been talking a bit about industry consolidation through mergers and acquisitions (M&As) in the video game industry as of late. The impetus for that discussion has been a series of high-profile acquisitions for several notable companies, namely Microsoft and Sony. Microsoft acquired Zenimax for $7 billion and Activision Blizzard King for a bonkers $69 billion recently, while Sony jumped into the game by acquiring Bungie for $3.6 billion. Of interest for these pages is the different approaches these companies have taken with these acquisitions. Microsoft hemmed and hawed about whether it would start building Microsoft exclusivity for products from its acquisitions, eventually landing on very much embracing exclusivity, while Sony took a much more hands-off approach and stated plainly that Bungie games would still be cross-platform. For those of us interested in digital and technology economies and business models, this is interesting stuff.
But there is a name missing here. The traditional "Big 3" in gaming has long been Microsoft, Sony, and Nintendo. Well, if you like real-world experiments when it comes to business strategies, this looks like it's going to get even more fascinating, as Nintendo is making noises about going an entirely different route.
While Xbox and Sony are entering an acquisition arms race, Nintendo isn’t so eager to snap up a slew of game studios. In a recent investors’ meeting, Nintendo president Shuntaro Furukawa was asked about acquiring game companies—a timely question, that’s for sure.
“Our brand was built upon products crafted with dedication by our employees, and having a large number of people who don’t possess Nintendo DNA in our group would not be a plus,” Furukawa replied, as reported by Bloomberg and Reuters.
Now, this shouldn't exactly come as a shock to anyone who knows the industry and how Nintendo operates. Whatever I might want to say in my series of posts about how "Nintendo hates you", the company has also built a successful business in the space that relies on first-party game titles and franchises compared with Sony and Microsoft. Whatever success those others have had, for instance, Microsoft and Sony simply don't have a version of the Super Mario Bros. franchise. Nintendo has several of these: Super Mario Bros., Zelda/Link, Star Fox, etc. So Nintendo has always been less reliant on 3rd party titles compared with its competitors.
But the open question is whether this more insular focus will work in the post-pandemic period where industry consolidation is not just for the video game industry, but for many others. The Harvard Business Review had a study released in 2021 that predicted what many others have as well: the mid- and post-pandemic economic space will be one that heavily incentivizes mergers and acquisitions. Consolidation is the order of the day/year.
So now we have three distinct strategies from the Big 3 of the video game industry: Microsoft will do M&As and try the exclusivity route, Sony will do M&As and be more open and permissive or cross-platform releases, and Nintendo will simply choose largely to not play this game at all.
At its core, Nintendo is not an enterprise built on corporate consolidation. It’s a company that makes hardware and games for said hardware. That is etched in its DNA.
And now we get to sit back and see how that works in a post-pandemic world.


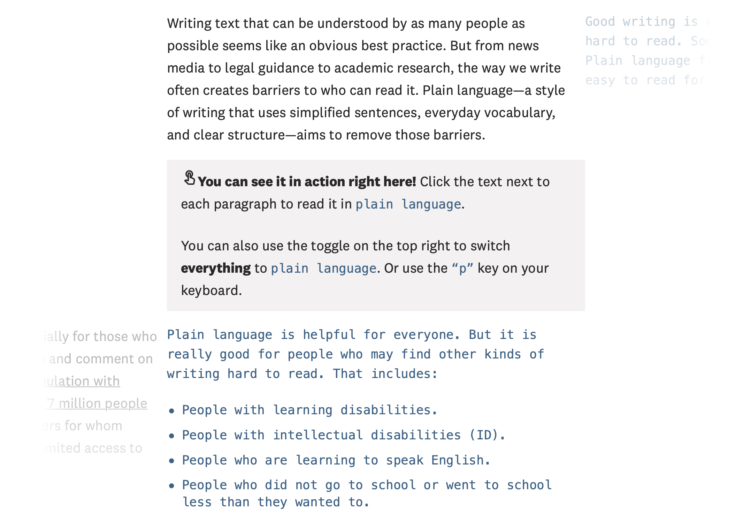






/cdn.vox-cdn.com/uploads/chorus_asset/file/23235492/1040294400.jpg) Fredrik von Erichsen/picture alliance via Getty Images
Fredrik von Erichsen/picture alliance via Getty Images
/cdn.vox-cdn.com/uploads/chorus_asset/file/23235499/1238354080.jpg) Dimitris Isevidis/Anadolu Agency via Getty Images
Dimitris Isevidis/Anadolu Agency via Getty Images

/cdn.vox-cdn.com/uploads/chorus_asset/file/23235799/GettyImages_1232074668.jpg) Jon Cherry/Getty Images
Jon Cherry/Getty Images
/cdn.vox-cdn.com/uploads/chorus_asset/file/23235988/GettyImages_1233962817.jpg) Craig F. Walker/The Boston Globe via Getty Images
Craig F. Walker/The Boston Globe via Getty Images







/cdn.vox-cdn.com/uploads/chorus_asset/file/23226676/GettyImages_1332009310.jpg) Chip Somodevilla/Getty Images
Chip Somodevilla/Getty Images
/cdn.vox-cdn.com/uploads/chorus_asset/file/23226702/GettyImages_1027064682.jpg) Chip Somodevilla/Getty Images
Chip Somodevilla/Getty Images
/cdn.vox-cdn.com/uploads/chorus_asset/file/23208238/temp.png) US District Court for the Northern District of Alabama
US District Court for the Northern District of Alabama


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}