
Shared posts
03 Jul 19:28
I’m Taking a Stance Against “The Pursuit of Lifelong Learning”
by Andy Brown
Let me explain.
First, I want to distinguish between “lifelong learning” and lifelong learning. The first is a phrase, the second a behavior. The behavior I have no problem with. It’s a prerequisite for staying relevant in a rapidly changing world.
But I’m taking a stance against the phrase. To tell me I should “pursue lifelong learning” is a fact. It’s obvious and offers me no insight. Of course I should pursue lifelong learning. I should also eat right and exercise. But how?!
I really struggled with this question in my first year of college. At that time I was not a pursuer of lifelong learning. Don’t get me wrong: I still learned. But I did it reluctantly. I learned in 12-hour sessions which ended 20 minutes before the start of an exam.
But not everyone was like me. I remember watching with envy as some of my impossibly-enlightened friends spent the night after (yes, after) the exam trying to figure out how to solve that one exam question they just couldn’t crack in the allotted time. These superhuman specimens of study baffled me. The exam was over! Why were they doing this?! At the time, I thought the answer was self-discipline. In hindsight, I see it’s even simpler.
They learned because they loved learning.
The fact that they pursued lifelong learning was true, but that behavior was a symptom of a much deeper part of their identities. They were learners. Of course they spent their time learning.
With time, I learned to love learning too. It didn’t happen overnight, but as college progressed my motivation to study became less about the grade and more about the satisfaction I felt when I discovered something new. I was becoming a lifelong learner.
Today, I’m lucky enough to work at Udacity--where taking online classes is a big part of my job--and my identity as a learner has only grown with time. Because as you learn, you build new mental structures to which you can more easily affix new learning. New learning creates new opportunities to form connections across domains that once seemed separate and these connections let you find simplicity in topics which once seemed complex. In short: as you learn more, you actually learn to learn better!
And if you love learning itself, this turns into an endless cycle. Because when you love learning, you do it. When you do it, you get better. And getting better makes you love it more. In short, a love of learning causes lifelong learning.
If you find yourself struggling to find the motivation to learn (lifelong or otherwise), consider reframing the problem. Instead of “how can I get myself to pursue lifelong learning?” try asking “how can I get myself to love learning itself?”
Neither problem is easy to solve, but the second sounds like a lot more fun.
First, I want to distinguish between “lifelong learning” and lifelong learning. The first is a phrase, the second a behavior. The behavior I have no problem with. It’s a prerequisite for staying relevant in a rapidly changing world.
But I’m taking a stance against the phrase. To tell me I should “pursue lifelong learning” is a fact. It’s obvious and offers me no insight. Of course I should pursue lifelong learning. I should also eat right and exercise. But how?!
I really struggled with this question in my first year of college. At that time I was not a pursuer of lifelong learning. Don’t get me wrong: I still learned. But I did it reluctantly. I learned in 12-hour sessions which ended 20 minutes before the start of an exam.
But not everyone was like me. I remember watching with envy as some of my impossibly-enlightened friends spent the night after (yes, after) the exam trying to figure out how to solve that one exam question they just couldn’t crack in the allotted time. These superhuman specimens of study baffled me. The exam was over! Why were they doing this?! At the time, I thought the answer was self-discipline. In hindsight, I see it’s even simpler.
They learned because they loved learning.
The fact that they pursued lifelong learning was true, but that behavior was a symptom of a much deeper part of their identities. They were learners. Of course they spent their time learning.
With time, I learned to love learning too. It didn’t happen overnight, but as college progressed my motivation to study became less about the grade and more about the satisfaction I felt when I discovered something new. I was becoming a lifelong learner.
Today, I’m lucky enough to work at Udacity--where taking online classes is a big part of my job--and my identity as a learner has only grown with time. Because as you learn, you build new mental structures to which you can more easily affix new learning. New learning creates new opportunities to form connections across domains that once seemed separate and these connections let you find simplicity in topics which once seemed complex. In short: as you learn more, you actually learn to learn better!
And if you love learning itself, this turns into an endless cycle. Because when you love learning, you do it. When you do it, you get better. And getting better makes you love it more. In short, a love of learning causes lifelong learning.
If you find yourself struggling to find the motivation to learn (lifelong or otherwise), consider reframing the problem. Instead of “how can I get myself to pursue lifelong learning?” try asking “how can I get myself to love learning itself?”
Neither problem is easy to solve, but the second sounds like a lot more fun.
http://blog.udacity.com/feeds/posts/default
Tribsantos likes this
12 Apr 02:29

Are Mammograms Worth It?
by Emily Oster
A Canadian study published in February reignited the years-long debate over breast cancer screening methods, arguing fairly strongly against mammography, or the use of X-rays to detect tumors. The study’s authors say mammograms have no survival benefit relative to physical breast exams and in fact lead to significant over-diagnosis. In their words: “The data suggest that the value of mammography screening should be reassessed.” Predictably, not everyone agreed with them.
The debate over mammograms centers on two questions. First, how many lives are saved by mammography? Or more specifically, how many tumors are detected early enough with this technology but would be missed by a physical exam until it was too late? Second, to what extent do mammograms increase over-diagnosis? Some small tumors will never be fatal. They will grow so slowly that within a normal lifetime, they will not cause illness. There is no reason to treat these tumors with chemotherapy or radiation since there is no survival benefit to doing so, and such treatments are unpleasant and carry their own risks. Mammograms increase the rate of over-diagnosis since they detect smaller tumors. The key question is: Do the possible survival benefits outweigh this over-diagnosis risk?
Every year, about 300,000 women are diagnosed with breast cancer and 40,000 die from it. Among the strongest predictors of survival is early detection: The smaller the tumor is when it’s identified, the better the woman’s odds of survival. This makes breast cancer screening — looking for tumors in women who otherwise have no symptoms — a central component of prevention. The simplest way to screen for tumors is a physical exam. But such an exam can only identify tumors that are large enough and close enough to the surface to be palpable. Because of these limitations, starting in the 1960s women and their doctors turned increasingly to mammograms, which use X-rays to find tumors at an even earlier stage of development.
The American Cancer Society recommends that women over 40 get a mammogram every year. Up until 2009, this was also the recommendation of the U.S. Preventive Services Task Force, an independent panel of experts appointed by the federal Department of Health and Human Services. But the task force changed its recommendation, saying that women between the ages of 50 to 74 should get a mammogram every two years. These conflicting recommendations from national organizations have muddied the waters for women around an incredibly common procedure – 67 percent of women over 40 have had a mammogram in the last year.
The recent study only added to this confusion. It was somewhat striking, to me at least, that it got so much attention, since no one should have been surprised by the results. The study was based on data from a large randomized controlled trial in Canada, which began in the 1980s and involved about 90,000 women. Half of the women were randomly assigned to have more or fewer mammograms.14 The other half engaged in physical exams only; younger participants were told to conduct yearly self-exams and older participants were given yearly physical exams by a doctor.
The mammography screening component of the study ran for five years. After that, the two groups could engage in whatever screening they chose (mammograms, physical exams, etc). In 1992, the first results from the study were published. After seven years, there were no differences in breast cancer death rates between the two groups.
In 2000, now 13 years out from the start of the study, more results were published, and again mammograms had no impact on these women’s deaths rates. It’s important to note that in this period from 1992 to 2000 the women were not receiving differential breast care, at least not as part of the study. The study was set up this way in order to answer the question of whether there were longer-term impacts of short-term screening.
The most recent study extended this follow-up to 25 years and, again, found no impacts. In my view it would have been surprising — not impossible, but surprising — to see no impacts 13 years after the study and then suddenly find impacts 25 years later.
Putting all of these results together, things don’t look good for mammography. It would be a shame to stop with this study, though, since it’s only one of many large randomized controlled trials of mammography. If we want the entire picture, we need to look at all of them together.
Most of the work is already done for us by Cochrane Reviews, which published on this topic in 2013. The Cochrane Reviews are a series of summary documents on a whole host of medical questions. Their goal is to aggregate information from individual randomized controlled trials to provide evidence-based guidance on best practices.
In the case of mammograms, the review in question aggregated eight large randomized trials encompassing more than 600,000 women. All of these trials had a similar structure to the Canadian trial: They divided women into two groups, and one group got mammograms with some frequency over a period of several years while the other group got “usual care.” The researchers then compared breast cancer deaths, diagnoses and treatments between the two groups.
One of the key advantages of these Cochrane Reviews is that they try to say something about the quality of each study they cover. In this case, the authors argue that three of the large trials were well-randomized and unlikely to be biased, and five were less well randomized and more likely to be biased. What it means to be “sub-optimally randomized” varies across trials, but to give one example: in a large trial in New York, which started in the 1960s, more than twice as many people with a history of breast cancer were excluded from the mammogram group than from the control group. This suggests more women with previous breast cancer were included in the control group, thus biasing the conclusions in favor of mammograms.
When we focus on the high-quality trials (the Canadian study is one of these), the Cochrane Reviews’ authors found those who were screened with mammograms were only slightly less likely to die from breast cancer in the seven or 13 years following the trial. This effect was not statistically significant. And, perhaps more important, they were no less likely to die overall.15
It’s not that mammograms do nothing. Women who were randomized into the mammography group were much more likely to be diagnosed and treated for breast cancer — this was true for all the studies. And it starkly illustrates the over-diagnosis issue. In the control group, some small tumors were not detected or treated, but they were detected in the mammogram group, hence the higher diagnosis rates in the latter group. And yet women in the control group were no more likely to die of breast cancer. This suggests those tumors that were missed were often not fatal.
Taking these results together, some doctors and policymakers have argued for a significant decrease in the use of mammograms — the argument being that the risks of over-diagnosis are too large.
Where you fall in this debate depends on whether you believe a mammogram really has no effect on survival or just that any effects are small — perhaps too small for studies like these to pick up. It also matters how you decide to trade off number of deaths versus number of unnecessary treatments. Is it worth one additional death to avoid 10 women being treated unnecessarily? Twenty women? Clearly, this is not something everyone will agree on, and there’s a good argument that the choice to get a mammogram should be left up to women themselves.
In my view, however, this debate ignores a more important question: How can we use the good information from mammograms without experiencing the risks associated with over-diagnosis? One of the central assumptions of economics is that more information cannot generate worse decisions. Mammography clearly provides more information. The problem is that contrary to our typical economic assumptions, it seems hard for doctors and patients to ignore this information. Once a tumor is detected, we want to treat it.
It is clear that watchful waiting would sometimes be a better policy. And there’s no practical reason we can’t have that policy; it’s a common treatment in the case of prostate cancer. In an ideal world, we could use better data to guide such a policy. What features of a tumor predict slow growth? Is there a threshold size and location of a tumor that should dictate treatment? Could more frequent mammography after a tumor is detected be useful? Rather than throwing away the technology, let’s see if we can better use it.
Tribsantos likes this
14 Nov 02:05
What the United States and Myanmar no longer have in common
by Chris Blattman
Countries that, as of 2012, did not use the metric system:
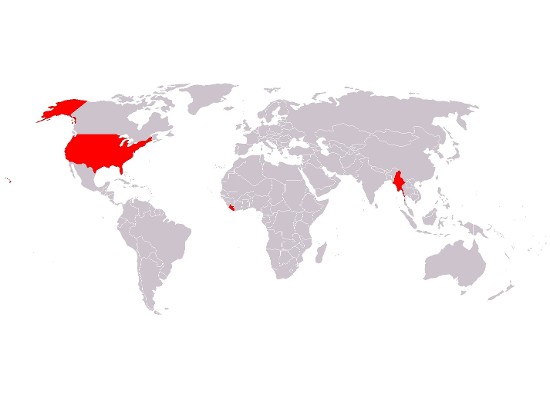
In 2013, breaking news:
Myanmar is preparing to adopt the metric system or the International System of Units (SI System) as the country’s official system of measurement, according to the Ministry of Commerce.
That’s right folks, the US and its former quasi-colony are the last hold-outs — and one of those two didn’t have a functioning government for most of the last three decades.
(The saddest part of that last statement is that it’s not obvious I am referring to Liberia.)
After living here 13 years I’m still getting accustomed. I now manage to think in miles as easily as kilometers, and I only seldom feel the need to convert Fahrenheit to Celsius in my head (though that’s partly because I’m bad at multiplying stuff by 5/9).
Even so, just last week I was trying to order large Ziploc bags on Amazon, thinking to myself “What exactly is a quart again? Sounds big. Sure, why not get the four-box pack?” *Click* Today I am awash in large-ish sandwich bags.
I’m curious what the political stakes are. Tragically, I suspect the average House member is convinced that such Obametrics are the fast path to socialism.
The post What the United States and Myanmar no longer have in common appeared first on Chris Blattman.
Adam Victor Brandizzi, Tribsantos likes this
12 Nov 04:04
There should be more female mayors
by Economic Logician
It is well known, and I have documented it before, that women behave differently from men in politics, in particular when it comes to policy priorities. While the various examples I have discussed before are interesting, it is difficult to ascertain that they generalize. Indeed, politics is fraught with social and local norms. We need more studies.
Fernanda Brollo and Ugo Troiano look at municipal elections in Brazil and concentrate on those where the mayoral seat was hotly contested between a male and a female candidate. One can thus consider that the electorate was essentially similar whether the female or the male won. The outcomes are damning for men. Whenever a woman became the mayor, health outcomes are better, corruption is lower, and the municipality gets more federal funding. To illustrate how men are politicizing relatively more, Brollo and Troiano find that male mayors up for reelection will hire many more temporary workers, a clear sign of electoral patronage.
Fernanda Brollo and Ugo Troiano look at municipal elections in Brazil and concentrate on those where the mayoral seat was hotly contested between a male and a female candidate. One can thus consider that the electorate was essentially similar whether the female or the male won. The outcomes are damning for men. Whenever a woman became the mayor, health outcomes are better, corruption is lower, and the municipality gets more federal funding. To illustrate how men are politicizing relatively more, Brollo and Troiano find that male mayors up for reelection will hire many more temporary workers, a clear sign of electoral patronage.
Tribsantos likes this
04 Nov 19:27
Let Anyone Take a Job Anywhere: My Closing Statement for IQ2, by Bryan Caplan
It's hard to believe we're even debating "Let anyone take a job anywhere." If someone said, "The law should prevent women from working," or "The law should prevent Jews from working," or "The law should prevent blacks from working," you wouldn't just disagree. You'd be appalled. You should be equally appalled when someone says, "The law should prevent foreigners from working." Criminalizing the employment of women, Jews, blacks, or foreigners is doubly evil. It denies the workers' basic human rights. And it deprives the world of the full benefit of the workers' talent and ambition.
Open borders should be a bipartisan, bi-ideological cause.
Conservatives should oppose immigration restrictions in the name of freedom, free markets, small government, the work ethic, meritocracy, and Horatio Alger himself.
Liberals should oppose immigration restrictions in the name of equality, reducing poverty, equal opportunity, non-discrimination, social justice, and the global 99%.
When the government forbids American farmers to hire Mexican farm workers, how can a conservative not see the oppressive hand of Big Government crushing the entrepreneurial spirit? When the government forbids American restaurants to hire Haitian dishwashers, how can a liberal not see a heartless legal system diabolically promoting poverty and discrimination?
Please! Let anyone take a job anywhere. It is the right way to treat your fellow human beings. It will transform the world for the better. And it will cost us less than nothing.
(13 COMMENTS)
Tribsantos likes this
![In a cavern deep below the Earth, Ayn Rand, Paul Ryan, Rand Paul, Ann Druyan, Paul Rudd, Alan Alda, and Duran Duran meet together in the Secret Council of /(b[plurandy]+b ?){2}/i.](http://imgs.xkcd.com/comics/ayn_random.png "In a cavern deep below the Earth, Ayn Rand, Paul Ryan, Rand Paul, Ann Druyan, Paul Rudd, Alan Alda, and Duran Duran meet together in the Secret Council of /(b[plurandy]+b ?){2}/i.")
No more posts. Check out what's trending.