Among the privileges of compiling these reports, is the opportunity to tell my own story:
I caught Corona very early, along with a lot of people I know. I was extremely sick with a very high fever for four days, but never hospitalised or anything like that. After the acute symptoms passed, it took me about three weeks to fully recover, at which point Germany had locked down.
I’ll admit that I found the panic propaganda convincing at first. I was never personally worried about infection – I assumed I was immune – though I did find the prospect of mass mortality and social chaos concerning. In retrospect, the propaganda worked above all by presenting the threat of Corona stripped of all context. What kind of social or political threat had past pandemics proven to be? (Answer: Not much of one.) How dangerous is SARS-2 really, compared to other viruses? (Answer: It’s no more dangerous than pandemic influenza, with which we’ve had abundant experience.) What precautions had been taken in the face of past pandemics? (Answer: Not many.) What kinds of countermeasures had our governments planned, and why? (Answer. Definitely not lockdowns, because they have no real chance of working.) These are all questions that went studiously ignored, but their import wasn’t obvious to me at the time.
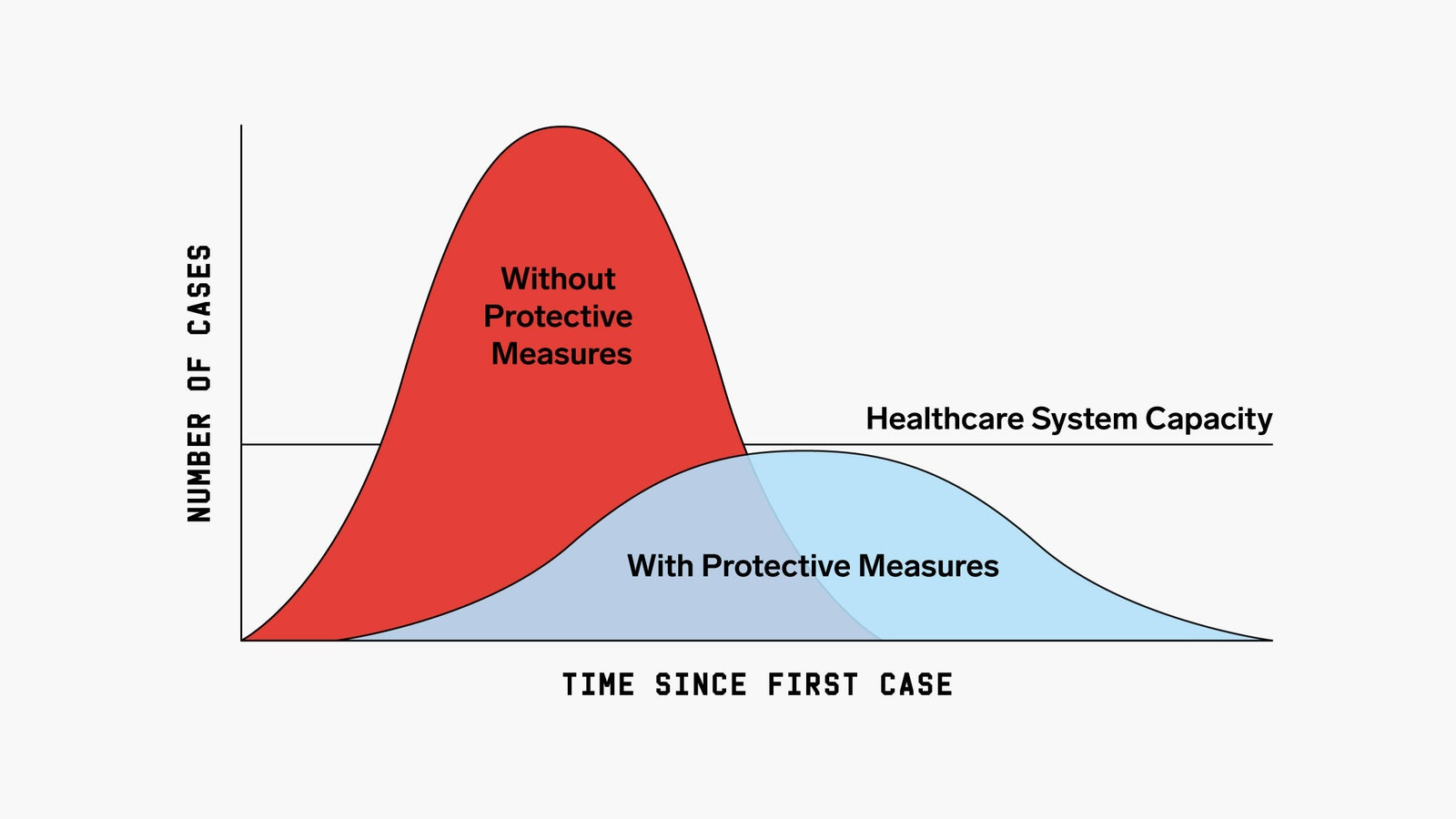
Like many of you, I was very interested in the Diamond Princess as a natural experiment, but by the time I had recovered enough to consume a lot of news, the narrative had shifted. Lockdowns were demanded not to save lives, but to reduce stress on the healthcare system, and above all to ensure the wide availability of ventilators.
There was no single event that convinced me I had been deceived, just a lot of little things. The first, was when disaster failed to materialise and infections began to recede towards the end of March. I found it hard to believe this could have anything to do with the German lockdown. It looked exactly like a seasonal decline, and the timing wasn’t right. By mid-April, it was clear that hospitals in Germany were never in danger of being overrun, and that ventilators were not any kind of answer to Corona. It sounds crazy to type it now, but the ventilator panic had formed a huge part of the argument for mass containment in those early days, and I was astounded to see a lot of lockdown hardliners continue to insist on widespread closures, now on the strength of totally different arguments. I also didn’t like the growing leftist flavour of containment activism, and the moral scolding of the press, which quickly adopted the tactic of blaming infections and deaths on individual rule-breakers rather than on the virus or our response.
The failure to dismantle containment over the summer; the obviously strategic choice of the press, beginning in August, to hyperventilate about cases rather than hospitalisations or deaths; and the remarkably low quality of public health messaging were all alienating. The final straw for me was the renewed panic over the entirely predictable rise of infections in Fall 2020. I’d always doubted that masks could do very much, but in the course of November it became clear that closures, too, had no detectable effect on the trajectory of infections. By December, I found it hard to see containment as anything other than a theatrical exercise, intended to drive the population into the arms of the vaccines.
This should have made me suspicious of vaccines from the very beginning, but here too I was slow. I thought they would, at the worst, be ineffective if harmless, and provide an excuse for our countries to disengage from containment. I could not have been more wrong, but here I saw the light much sooner. As politicians and media outlets portrayed another seasonal decline in infections as a victory for the vaccines, I was on guard again. The increasingly toxic, bullying information campaign surrounding vaccination didn’t help, and the ever more frequent reports of adverse events soured me on them entirely.
Many academics in fields well outside public health and epidemiology wrote about the valuable perspective provided by their own areas of expertise.
Procopius, a pseudonymous Argentinian professor, reports that it was above all the relentless “threat inflation,” familiar to him from his work on international security, that clued him in that something was wrong:
For me, the wake up moment was early on, more or less around March, when my country decided to plunge itself into an early hard lockdown.
Since my area of study is international security, I follow international news outlets very closely, so I got on to the covid subject early on.
In late February or early March, at a meeting with other academics in my field, I was asked to give an overview of relevant situations unfolding around the globe. At the time I had already come to the conclusion, based on several early data points (South Korea’s reported IFR rate), that the threat was overblown. I risked an early forecast that this would be a an episode similar to the 2009-2010 swine flu scare, but shorter in duration, since we supposedly had learned our lesson from back then. After all, other scares like Ebola, Zika and Chikungunya had blown over much more quickly since then.
Needless to say, my forecast turned out to be spectacularly wrong, and this pushed me to dig ever deeper into the informational environment surrounding Covid, trying to understand why.
My greatest worry then was that the media circus around Covid would push people to stay home, which might cause an economic downturn in an already struggling economy, that our chronically inept government would find difficult to counteract. I never thought the government of our poverty-stricken country would so happily jump on that risky bandwagon of global policy, yet they did.
One red flag that caught my attention early on was threat inflation. Those with knowledge of security issues should recognize the problem immediately, because it is so pervasive in our field. National security bureaucracies have a vested interest in inflating the threats they are facing in order to justify their budgets, prestige, and their powers.
We can see this at work in the war on drugs, human trafficking, military force posture planning, even nuclear strategy. The worst offender is, by far, the global war on terror since 2001. All the mentioned threats are real, which is why they are plausible at face value, it just their likelihood and severity that are grossly exaggerated.
And the hygiene theater around covid strongly resembles the security theater around terrorism, where most policy measures are meant to show action without actually being effective (or even counterproductive).
My ignorance about the workings of the public health establishment led me to overlook the danger of these dynamics playing out the same way during this pandemic, with even worse effects on a global scale. And it makes one wonder what other industry-bureaucracy collusions are waiting for a golden opportunity to force their pet projects on the rest of society (yes climate change, I am looking at you!)
Needless to say, as a result of all this, I was already skeptical of the vaccination efforts from the beginning. It was obvious that there was no way to assess long term side effects because there would be no time, period. And there would be immense pressure to cut corners and weaken regulatory oversight. The half-baked PR stunts to discredit ivermectin and HCQ strongly suggested pharma lobby and regulatory capture.
On a final note, working in academia I have long been aware of how our scientific production system has to a large extent been corrupted by perverse incentives to become a paper mill.
I used to think this was mostly a social sciences problem, but after Ioannidis (2005) I increasingly learned how deep the problem went into the supposedly hard sciences as well. If the average citizen were more aware of this, they would probably be much more wary of worshipping at the altar of The Science!
My friend, the physicist Rudolph Rigger (he writes Riggery Pokery), realised that mortality curves for the United Kingdom tended to decelerate far too early for lockdowns to be the cause:
I’m a theoretical physicist with over 30 years research experience. My work has almost exclusively involved squiggles – figuring out math stuff to try and tease some new physis idea out of things. I wasn’t so good with data and stats because I didn’t need to be – the confounders tended to confound me every time. I’ve learned quite a lot over the last 20 months or so, but I’m still a bit slow with the data analysis. I say these things to give an honest contextual frame from which you can evaluate my comments. It is very clear, that other than naïve basics, I am neither an immunologist, or an epidemiologist.
I was working at a university away from my country of birth (the UK) when the dread Rona struck. I remember some of my colleagues trying to push the elevator buttons with their elbows and thinking this might be taking things a tad too far. To be fair, I didn’t know much about things back then, but I doubted very much whether infection from surfaces and objects would be significant – more of a theoretical possibility than any serious risk. The country I was working in followed the rest of the world and eventually imposed lockdown, but I followed the UK situation very closely.
I thought the idea of lockdown was a bit silly, even sillier was the notion that asymptomatic transmission could be a significant factor. Lockdown was just going to be a tool for delaying the inevitable (back then I thought it might “work”) and my naïve understanding of immunology and infection was that if you have sufficient viral load to pose a significant danger to others, you’re going to be experiencing symptoms. I wasn’t sure what lockdown of healthy people was going to achieve over and above “locking down” people with symptoms. I also knew from the Diamond Princess data and the data from Italy that, whilst serious, the situation did not really qualify as an “emergency” for the majority of the world’s population. So lockdown seemed to be a bit of a panic-induced over-reaction.
As things progressed I looked at the UK data a bit more closely. The mortality curve rose, reached a maximum, and then started to come back down again. Well knock me down with a feather, I thought, lockdown actually worked. I wanted to find out when lockdown actually started to “bite” so I started looking at the properties of the curve. In physics and maths you have to delve into the deeper properties of curves if you want to understand them properly – you have to look at things like first and second derivatives. The 2nd derivative is especially important in understanding dynamics because it’s a measure of “acceleration” – it tells you when the brakes are on, so to speak. In physics, accelerations tell you something about the forces that are operating. I worked out, from the data, a decent approximation for this “acceleration” for the UK covid mortality curve – and shifted by a couple of weeks to get an idea for the dynamics of the infection curve (death followed infection by at least a couple of weeks on average).
To my surprise, I found that the acceleration for the infection curve had gone negative (the brakes were on), BEFORE the lockdowns could have had any effect. This strongly indicated, but did not absolutely prove, that the viral dynamics were being driven by natural processes of a virus within a population and largely not affected by policy. From that point on I started to look much more closely at the data across the world, noting geographical/climate patterns, and also noting that there didn’t seem to be a good correlation between policy and outcome. When mandatory masking was introduced in the UK Summer when things had seasonally fizzled out I knew something was very wrong. As a vaper, and having to wear masks in the country I was in, I knew that masks were going to do bugger all, to use a technical term.
One and a half years on my position has only been strengthened by the worldwide data. Almost everything the media and “the powers that be” were telling us was, at best, a distortion of the truth and, at worst, an outright lie. The ramping up of censorship, and the application of various labels like “anti-science” or “science-denier”, only confirmed my feeling that everything was being driven by emotion, rather than data. We were being emotionally manipulated to think and behave in a certain way. What I’ve not been able to figure out is why. Very little about the response to this virus makes sense from the perspective of public health, or evidence-based policy. We’ve not been following science, we’ve been following beliefs.
An orthopedic surgeon from the midwestern US is one of various doctors who were struck from the very beginning by the futility of containment. Direct knowledge of a vaccine-induced death, meanwhile, convinced him that the vaccines were a bad idea very early;
Our hospital went into lockdown in late March 2020. I knew something wasn't right immediately because there were no patients with COVID in the hospital. Our hospitals were empty, but I could not take care of my own patients as all elective surgery was cancelled. Very quickly the hospital realized that they were going to go bankrupt, so we came back to work in 6 weeks and worked pretty much a normal schedule since. It was not a coherent strategy.
One of my initial responses to the lockdown was to share the story "The Mask of the Red Death" by Edgar Allen Poe with all the physicians in training that I surpervise. The similarities were too obvious. I told them "it's a virus. You can run and you can hide, but eventually we are all going to get it."
When the vaccine was first announced, I found a review paper on mRNA vaccinces from 2018. It described the 30 years that scientists had been working on mRNA vaccines. I read about all the problems and thought it was a might odd coincidence that they worked out all the bugs just in time for COVID and an EUA. I decided to wait and see how the role out went. Then in March of 2021 a local 16 year girl who was a friend of my son died from a pulmonary embolis after vaccination. And it was not reported in the media. I vowed then and there NEVER to get the vaccine. And I have manage to keep my job despite the mandates - it just takes resolution ( and perhaps being a big biller for the hospital).
Various people with an insider perspective on the pandemic response wrote in. It’s good to know that the vaccination campaigns look as bad from the inside as they do from the outside:
I worked in one country’s vaccine national roll-out program….I started in their adverse event team…
I could list more as a member of the public but from within the vaccination program:
-When the pharmacovigilance advisors complained about the reporting of the AEFI [adverse events following immunisation] system and why it was not a true phv [pharmacovigilance] reporting system and completely inadequate.
-When they complained that their recommendations based on their research and calls with other countries were ignored (e.g. they had zoom calls with Israel and WHO over the booster roll-outs and Israel initially did it for solely political reasons….there was no data to support doing it).
-When the country sat on publicly announcing a vaccine death for 3 to 4 weeks, because we had entered another lockdown and they didn’t want to deter people from getting vaccinated.
-When they ran an active monitoring text survey on adverse effects to randomly selected people who had doses….but the then.director of the program said not to publish the data, as the reactions were so high.
-When I realised there were 55 people employed to do communications within the program….aka keep up the narrative from the government ….
Eileen Natuzzi, a physician and epidemiologist who also writes on Substack, found the response bizarre from the very beginning:
I worked for the department of public health spanning the pre- and post-vaccine COVID period. I am a physician and a public health epidemiologist. Before the vaccine it was about collecting info from cases, no emphasis on education or allaying media stoked fears. The vast majority of cases were mild but terrified. We failed to separate ‘died with’ from ‘died from.’ There was no stratifying cases by severity of symptoms even though that data was there. The mantra was “just collect the data.” As a physician this made no sense to me. I went rogue recommending Vit D, C, zinc and early monoclonal Ab treatment for the high risk. It was not our policy to do so.
Then came the mass vaccine period, the shifting of human resources in order to jab the population. Any mention of adverse events was met with: “are you trying to sabotage the vaccination campaign?” There was no critical thinking, no unbiased looking at information, it was forge ahead with the mission at all costs. By February and March 2021 the over interpretation of vaccine benefits began: “look at how the cases dropped off once the vaccines were available.” Nope, look at how cases have also dropped off where vaccines were not available. It’s due largely to the virus’s behavior not the vaccines. Our public health bureaucrats have given far too much credit to the vaccines, magical one sided thinking, no objective data analysis. Just look the other way and keep jabbing. Once public health crossed the threshold into biased analysis I was out, tendered my resignation. The system was incapable or unwilling to see the slowly rising breakthrough cases, to understand them, they just buried them. It was quite disappointing and it reinforced to me that a public health overhaul is sorely needed. An overhaul must include a commitment to the individuals they serve, not control, to provide honest up to date data and information. Breakthrough infection data should be as upfront as case and death data, not buried on some obscure page of the local public health website. That is the type of transparency needed especially now as vaccines are failing to eliminate the virus. Public health must be put in a continuum with our illness system so patterns of concern become visible. There is no logic to having separate ineffective systems when one could compliment and perhaps even correct the other.
There is going to be a lot of data to dredge thru after this pandemic is over. Will the honest data be made available? Will it’s analysis be accurately interpreted or will some of the spin we are continuing to see taint it?
An anonymous reader with first hand experience of the SARS outbreak in 2003 found himself immune to the second round of hysteria in 2020:
I played a bit role in SARS Season 1 in Shanghai back in 2003. I went through the pantomime of containment of that bygone age, complete with lockdowns, hose-downs, temperature taking and effective-action faking. It was political theater of the highest order. Before the virus even hit the local news media, we already knew it was extremely difficult to pass and required little more than attention to some basic flu season hygiene. And then it was gone, thanks to the Wisdom and Leadership of Comrade Jiang Zemin and the Chinese Communist Party.
When Season 2 was released in late 2019 (I brought back COVID from China to the US in September of that year incidentally), it seemed to me a poor rehash of Season 1. More transmissible, yes, but inversely proportionally in terms of virulence. You could tell, however, they'd been rehearsing for S2 for a long time, almost dumbstruck their moment on stage had finally and truly arrived. Before it even hit our shores, it was evident this was a highway to authoritarianism - it worked so well in China twice, how could it not be employed here, in Europe and Oceania? From the start I asked: where are the exit ramps? There were none. Two weeks to flatten the curve. Uh huh ... have the troops home by Xmas (Korean War) ... over in a matter of weeks (WW I). History is replete with similar examples and their total failure to communicate an end to containment and what a post-lockdown world would look like only affirmed by suspicions; the St. Floyd riots were simply the mustard on the sh*t sandwich I knew we would be force-fed for as long as they thought they could get away with it, which places like Austria, Canada and Australia are demonstrating could be a very long time, indeed.
An Irish reader, who experienced the first year of the pandemic in China, before returning home to work as a contact tracer, offers many interesting observations:
I worked as a contact tracer here in Ireland for seven months (from February 2021 to September 2021). The contract tracing centre that I worked in was set up in late October or early November 2020. One of the things that I found out that shocked me was that before I joined, one of the contract tracers tested positive for Covid. This was hidden from the other contract tracers and no one working in the contact tracing centre was officially recorded as a close contact. One of the tracers found out eventually and sent a strongly worded email to everyone who worked there calling out the hypocrisy. Managers went round to everyone and told them to delete the email and nothing was done regarding isolation or testing of that worker’s close contacts.
This shocked me, because if the people telling the public to restrict their movements or self-isolate weren’t doing it themselves, then obviously the risk wasn't that great.
Another thing that convinced me that it was a scam was that there was no advice as to what to do when people tested positive. We had a huge script along with a scenario manual to tell us what to say to close contacts depending on their individual circumstances. Some of the close contacts we called happened to already have tested positive. They would ask me for medical advice. Perhaps it was for the best for non-medically trained contact tracers not to give medical advice, but I find it odd that the only response we could give was "Contact your general practitioner if your symptoms worsen".
*
I lived in China from November 2019 to November 2020 and if I remember correctly, China closed its borders and stopped or rerouted nearly all flights in February 2020. They had, and still have, very strict entry requirements when it comes to testing and quarantining. I remember thinking to myself in the early days that since Ireland is a small, sparsely populated, island nation that it would be able to successfully isolate itself from covid, at least relatively speaking. Ireland didn't do much regarding entry requirements until March, 2021 when they introduced a mandatory hotel quarantine, a whole year after the virus emerged. There were also lots of issues with the hotel quarantine. People challenged it legally, and many simply left the hotel after being checked in. Mandatory hotel quarantine was removed completely in September 2021. Perhaps this says more about the incompetence of the Irish government than anything.
I flew back to China via Hong Kong and London. On my flights to Hong Kong and to London the passengers were socially distanced. Every row at least was only occupied by one person. However, on my flight to Dublin from London every single seat was full! And there was no testing requirement to enter Ireland. While I didn’t care all that much as I had realised through browsing subreddits such as r/China_Flu and r/Wuhan_Flu that covid was only dangerous for people with comorbidities, I thought it was the height of hypocrisy as politicians in Ireland and the media fearmongered about the virus 24/7. The country that I came back to was and still isn't the same one that I left. It felt like the population was traumatised.
An American reader who helped coordinate the state-level Corona response recounts multiple red flags:
I was appointed to the Governor’s Covid Task Force for one of the 50 United States on March 23, 2020, and within two weeks it was clear there were considerable differences between what we were experiencing on the ground in our State and the direction of the Covid narrative in the media. At first we were mostly confused: why was one set of numbers—Covid cases—the singular focus of the narrative when there was so much context that was necessary to understand that number, even as a leading indicator? It seemed no one in the public narrative was asking any of the critical questions necessary to determine the real extent of the problem, they were simply churning the fear barrel as hard and fast as possible.
A critical question in our minds: If cases were a leading indicator of hospitalizations and deaths, how accurate were predictions of the progression from cases to hospital to death? In our State, we realized by April 7, 2020 that the publicly available models of the progression were far too pessimistic. We were also confused why no one was pointing out that the people who were dying were nearly all very old and/or very sick. Public Health Officials knew that age and co-morbidities were critical in determining the seriousness of this new disease but were being nearly ignored in the public narrative. Furthermore, why was no one pointing out that those who were not very old or sick were mostly obese. Those were not negligible factors, those were critical diagnostic variables that were being ignored.
At the time, the Task Force had to make decisions in the middle of that massive public fear narrative. While some of us on the inside seriously questioned most of what the public believed to be the “truth” about Covid, the Task Force itself (as well as the Governor) had to deal with the significant public pressure to go along with what other States and Governors were doing. By Governor’s order, we shut down the State in mid-April for four weeks “to flatten the curve” because that’s what virtually every other State in the country had done.
During that shutdown, because of the significant differences we were already seeing between the reality on the ground and the national narrative, Task Force insiders began to seriously question nearly all of the conventional Covid wisdom with basic decision-making questions, like:
· Differential deaths—how many people would normally have died by this day in the year versus how many have died this year? We needed to know whether the people being killed by Covid were mostly so old and/or so sick they would have died anyway. While it sounds callous, Public Health is about exactly that type of question.
· How critical was obesity? We have one of the five most obese populations in the United States, particularly among young people. While it may be politically incorrect to mention, it was the single most responsible question we could ask.
· How many people were hospitalized or died WITH Covid as opposed to OF Covid? We quickly realized national Covid case/hospital/death counts included gunshot wounds, cancer victims and a host of other injuries that had nothing to do with the virus. But federal reimbursement if there was a Covid diagnosis meant providers had a financial incentive to classify everyone who died WITH Covid as a Covid death, which made it difficult to determine this critical information.
Unfortunately we were unable to get the answers to most of those questions because the noise from the fear narrative was so great that non-compliant questions were simply not allowed (or actively suppressed). We did our best to actually fight the Covid fight on the ground, but our intelligence seemed to get worse because the fear narrative became both defensive and aggressive—they did not questions like these being asked, much less answered.
My personal journey was highly influenced by the national mask narrative. I was in charge of purchasing PPE, so when I joined the fight in March I studied everything I could about masks—how they were made, what the certifications were, who tested masks, what various markings like N95 or KN95 meant, etc. While doing everything I could to purchase and distribute as many masks as possible, that research began to make me doubt the effectiveness of most masks against Covid, especially for the general public. By early June I knew that the “my mask protects you, your mask protects me” tag line was completely false—masks are designed, tested and certified to protect the wearer and no one else. Since that line was being used by the same people telling us Covid was the “most dangerous disease of our lifetime” and the only way to combat it was with containment, I knew that they could not be trusted. Ironically, by June I was engaged in buying tens of millions of masks, knowing that they were unnecessary for Covid given its aerosol nature and the lack of discipline exhibited by most mask wearers.
The final straw for me was when the people screaming loudest for containment (in addition to lying about masks, case/death counts and Covid risk among the young) proudly flouted all their own mandates by participating in crowded, mostly maskless “racial justice” marches across the country. You only have to beat me over the head with hypocrisy for a little while before I finally wise up.
A journalist, medical writer and former medical school administrator was put off, above all, by the mass vaccination campaign:
Here briefly are the issues that made me a skeptic of the United States government's approach to the pandemic:
1. The campaign to vaccinate all adults was a giant red flag for me. It was clear from the beginning that this virus had an unusual J-shaped morbidity and mortality curve, not the more common U-shaped curve. Therefore, the emphasis should have been on vaccinating the older age cohort as well as those who had other serious diseases, especially ailments that compromised the immune system.
2. Related to this was the decision to vaccinate healthy children. I actually did a calculation about a year ago based on published CDC data and discovered that of the 73-million people in the U.S. in the 18 and under age cohort there had been less than 500 deaths, virtually all among children with other underlying serious diseases. This death rate for children works out to about .00000685 percent. Then I read studies -- first from Iceland and then from other countries -- that found that infected children were very unlikely to spread Covid19 to adults. At this time, using the flawed VAERS data, I calculated the risk of a child dying from the vaccine. It was, of course, very rare -- but slightly less rare than a child dying from the disease itself. I said to myself, surely they won't want to vaccinate healthy children. When the CDC approved vaccinations for healthy kids -- even preschool age children -- I said to myself, this whole system is corrupt. There was apparently not one person in a position of authority within the CDC willing to stand up against this nonsense.
3. Now we have reports of young men having serious cases of myocarditis, and some even dying. Nobody seems to care. It doesn't fit the narrative so the stories are ignored. The CDC takes no action. This heightened my skepticism of the whole government approach to the pandemic even more.
4. Dr. Fauci continues to spread lies and half-truths. But, one example: He initially said, truthfully, that a cloth mask offered some minimal protection for other people from an asymptomatic infection that the person wearing the mask might have. Later he started to lie about the effectiveness of these types of masks in protecting the wearer.
These are just a few of the things I could cite, but they are some of keys to how I began to become aware that there was a scam afoot.
I believe that the CDC and public health officials in the United States have damaged their credibility so badly that it'll take a generation for them to regain public trust. This was totally unnecessary. All they had to do was to level with the citizenry. Tell them about the complexities of the pandemic. For instance, they should have made clear the age differences in risk. They should have emphasized the concept of relative risk. They should have pointed out that though vaccines administered to at-risk groups does reduce those individuals' risk, they may actually increase the the likelihood of significant mutations, and hence, might pose additional risk for the population as a whole. These are complex matters and one has to weigh various risks against one another. The CDC knows this, but for whatever reason, decided the public didn't need to know everything -- but just selective information that would support the narrative they had decided on. In a word their behavior was and is shameful, not to mention paternalistic, in the worst connotation of that term.
A former US Marine Corps officer provides a military perspective. For him and many others, shrill warnings of impending disaster followed by nothing proved decisive:
I recently left the Marine Corps for the civilian world but back in early 2020, I was an officer in a combat arms unit stationed in California. Our unit was scheduled to deploy to the UAE for four weeks for a training exercise with the Emirate military beginning in March. In late February, a small group from our unit went to the UAE as an Advanced Team to prepare for the arrival of the rest of the unit. We heard about COVID on the news but didn’t think it was a serious threat at the time… if anything, we were more worried about the anthrax vaccines we had just received in order to be medically ready to deploy to Central Command.
The rest of us were scheduled to deploy around mid-March, but the Department of Defense canceled our deployment as we were sitting on a runway waiting to leave California. Fast forward a week and we find out from our higher command that they were scrambling to figure out a way to get our Advanced Team back from the UAE, but they probably wouldn’t come back for another three to six months. At this point we all knew COVID was something serious.
In late March, back at our base in California, the base Commanding General issued warnings that all units needed to prepare for a massive wave of COVID cases that would far exceed our base’s hospital capacity. The now infamous Imperial College of London COVID death projections were used as the foundation for our base’s own COVID preparations. We were further told that a M.A.S.H. style tent hospital was being constructed on the base to accommodate the inevitable mass-casualty event COVID was going to cause. Estimates stated that 50% of the base’s military and civilian population would be hospitalized by the initial wave and that most of those hospitalized would likely die. We were told that the civilian population surrounding the base may turn hostile once resources began running out over the coming months. The base began preparations for food and water rationing and units like mine were told to begin preparing our Chemical, Biological, Radiological, and Nuclear (CBRN) protective equipment for real-world use.
Then, nothing happened. From late March to July our unit of roughly 1,000 Marines and sailors had zero COVID cases. Zero. Even when we did have our first case, that individual felt sick for a day or two and then was fine. By late summer I realized that our local base narrative had changed from “we are all going to die” in March/April to “we need to do our part to keep hospitals from filling up” in April/May to something more like “although most military service members are not threatened by the virus, we all need to do our part to not kill the elderly in our surrounding civilian communities.” At that point I finally understood what many of my Marines had already intuited… COVID was no more serious a threat to us than a flu season. I regretfully understand now that I was in the middle of the intelligence curve for the first six months of COVID.
A US government employee with experience of the Defense Department writes that it was the creepy, coordinated internal messaging that caused him to question containment:
What really struck me in late Feb/Early March 2020 was the tone and content of messaging in internal emails addressed to staff members. I can only describe it as fake and creepy with the same sanctimonious air that usually accompanies other "politically correct" bureaucratic priorities. This was in late February, before the public really was exposed to this hysteria and the states began their lockdowns.
I knew immediately that something was pushing this, that the fear of COVID wasn't natural or spontaneous, and an official playbook had been developed. This playbook would reward those who furthered this agenda and punished those who stood in its way. The messaging was uniform and used certain words like safe, care, protect, etc etc. Within a couple of weeks, this new doctrine had been accepted as gospel by the entire managerial establishment at my government workplace and any naysaying or doubting of the narrative was absolutely unthinkable.
From the earliest days, this containment ideology was imbued with, not just a medical aspect, but a moral one. Failure to comply, and not only comply, but actively promote COVID ideology and work it into your plans and programs and inspire fear (i.e., "safety") in others would be tantamount to betrayal of the greater social justice ideology our government exists to promote.
As I write this, I am wearing a mask 100% of the time indoors again, after being forced to take a vaccination against my will. There are murmurs of forced boosters despite all we know about non-sterilization and omicron's immune escape capabilities. They won't let go. It's not about science anymore. They won't let us be free. I pray something or someone puts an end to this madness.
Finally, while I’ve tried to highlight interesting or less usual perspectives in these posts, the most instructive thing for me has been reading the literally hundreds of notes from ordinary people. I regret that I can’t publish them all.
No few Christians, Jews and Muslims have written that their faith played a key role in keeping them out of the pandemic hysteria, and their perspective is very important, in view of a hysterical response that has been driven above all by secular liberal societies:
We have known Jesus for 38 and 32 years respectively. In that time we have learnt to hear His voice, and have had long experience of God's ways with us personally, and the world.
I had Chinese students in my English class at our local university, here in Germany, in January 2020, all of whom wore masks when they entered the lecture room, and although I knew that the Chinese have worn masks in China for years, I was surprised that here in the West, they also did so. It got me thinking. I've been a reader of Zero Hedge for some years and when I read an article about a virus which had escaped from Wuhan and that a scientist there had been involved in bat research in 2019, I was suspicious.
I spoke to my husband about it, and shortly afterwards, God spoke to my husband
and told us that the panic over the virus coming from China was a lie and that we shouldn't be influenced by it.
Knowing this has given us peace throughout the last two years, although we have had very little work, our savings have all gone, we are now living hand to mouth - and even collect bottles and cans with deposit on them in order to buy a little food.
We know God is allowing this to effect His plans - we walk by faith in Him every day that He will provide for us (Job 13:15), we are grateful for the opportunity to be able to be a witness to the truth - that perfect love casts out fear - (1 John 4:18) and that knowing God is security and eternal life (John 17:3).
In my prior post, I mentioned that frequent travellers seemed uniquely immune to Corona hysteria. Felix R. Savage reports on his perspective, moving from Tokyo to the American South in early 2020:
Lifelong expat, deeply religious, no television, frequent traveller, sci-fi writer ... it's a mystery I fell for the Covid = Black Plague hoax at all. I did, though, from January-March 2020. During that time I moved my family from Tokyo to the Deep South (the move had been years in the planning). So we saw the panic campaign implemented twice over, once in Japan and then a couple of months later in America. I remember being strongly put off by the spooky lockstep similarity of the messaging. I have been travelling back and forth between Japan and the US for years. Never before had I seen any event framed identically in both countries. This time, it's like the Japanese and American media had both been given the same script. It was freaking creepy. (I still think this needs more explaining.) By March I had begun to notice that people were not, in fact, dropping like flies around us. […]
Painfully stupid hygiene regulations, from illogical mask rules to senseless plexiglass barriers, have done more than a thousand bloggers ever could to discredit the Corona circus:
I first realized this was a sham with the plexiglass barriers that went up all over... they hung from the ceiling in front of the cashier at the grocery store and I thought, "This virus is so smart and can see and can move itself around so well that it will stay on the proper side of plexi sheet?"
That seemed ludicrous to me. Grocery stores never closed, yet there are NO stories of Piggly Wiggly staff decimated by corona virus. There are NO stories of Home Depot stores being "superspreading" locations of death.
It's been nuts from the start.
And here at the bottom: Thanks again to all of you for writing in, and I’m sorry I couldn’t include more. Reading and editing your reports has been a fascinating experience, and I’m eager to continue this series. Soon I’ll ask you to submit updates on containment in your respective countries, but if there’s other topics you’d like to see featured, please let me know – either in comments, or via email (containment@tutanota.com).














{kind=link}