Devastating news: Walter Williams died last night (or early this morning).
Walter has been my colleague and friend for more than 35 years. He is one of my few heroes. I will write more later, but I am now in no condition to say more.
Devastating news: Walter Williams died last night (or early this morning).
Walter has been my colleague and friend for more than 35 years. He is one of my few heroes. I will write more later, but I am now in no condition to say more.
BIDEN, INC. IS A MAJORITY-OWNED SUBSIDIARY OF THE CCP: Uyghur Leader: We’re Worried About A Biden Administration. “With Tony Blinken poised to take the helm of the State Department in the Biden White House, Hudayar said U.S. support for the Uyghur people appears in jeopardy considering Blinken’s past statements in support of the Chinese crackdown on the minority Muslim population where the government claimed it was combating terrorism prior to constructing concentration camps. Millions of Uyghur people remain in such camps today.”
OH: Facebook’s bots ban thousands of small businesses from advertising at height of retail season.
The genius of the internet is that it created a level playing field where one-man shops could compete toe-to-toe with established players.
The evil genius of social media is that it allows established players to snuff out the one-man shops before they have a chance to compete.
A few weeks back I wrote an article about how high the risk of dying from covid is. I mentioned that a senior representative of the World Health Organization (WHO) had recently said that the WHO’s best estimate was that roughly one in 750 people who get infected die of the disease. I also mentioned a study published by the WHO, authored by professor John Ioannidis at Stanford University, which was based on antibody data. That study estimated that the mortality rate for covid was around 0,23% overall, which would mean that roughly one in 430 people who are infected overall die of the disease, and 0,05% for people under 70, which would mean that if you’re under 70, the risk of dying of covid is about one in 2,000.
Since then, professor Ioannidis has updated his figures. The newer numbers have been published in The European Journal of Clinical Investigation. The modifications have been made to compensate for the fact that the earlier estimates were extrapolated from the countries that were hardest hit by covid. When this is accounted for, the new estimate is that covid kills around 0,15-0,20% of those infected, so around one in 600 infected people die of the disease overall. Among people under 70 years of age, the revised estimate is that 0,03-0,04% die, which is around one in 3,000.
However, professor Ioannidis also mentions that the fatality rate varies a lot between countries, related to varying levels of risk factors. As I mentioned in a previous article, the main risk factor for dying of covid is obesity. So countries with high levels of obesity will be hit harder than countries with low levels, which likely explains why the US has been hit so much harder by covid than Japan. Other health related factors that increase the risk of dying of covid are high age, organ transplantation, uncontrolled diabetes, chronic obstructive pulmonary disease, liver failure, kidney failure, and cancer. Basically, the things that predispose you to dying in the near future more generally, also predispose you to dying of covid.
In his article, professor Ioannidis mentions attempts that have been made to estimate the number of years of life lost, on average, when someone dies of covid, and I think this is interesting to explore further, because it is actually extremely important when trying to determine how severe covid is. When a small child dies, for whatever reason, that generally means around 80 years of life are lost. If a 90-year old dies, for whatever reason, that usually means at most a few years of life have been lost. Most people therefore reasonably think it’s much more tragic when a small child dies than when a very old person dies, because much more potential lifetime has been lost.
So, if covid results in 20 years of life lost on average, that’s reasonably about 20 times worse than if it results in one year of life lost on average. And that’s why it’s important to know how many years of life are lost to covid, when someone succumbs to the disease.
So, how many years are lost?
An article was published in The Proceedings of the Nationol Academy of Science (PNAS) in July that sought to estimate this. Using cohort life tables (the tables that insurance companies use to predict how many years of life someone has left based on how old they are), they calculated that the average person who dies of covid loses 12 years of life!
To me, this number seems implausibly high, because it doesn’t match what I am seeing here in Sweden. Half of Swedish covid deaths happened in nursing homes, where median life expectancy is less than a year. If half of all people who died of covid in Sweden would have been dead within a year even without covid, that would mean that the other half who died would have had to have twenty plus years of life left, in order for the average to end up being 12 years.
Considering that the average age of those who have died of covid in Sweden is 84, while the average age of death in Sweden more generally is 82, that seems extremely unlikely. Just looking at the data from what has actually happened in Sweden, it seems more likely that the average amount of lifetime lost to covid is very low, a few years at most.
In fact, I would go so far as to venture that covid can not possibly have resulted in an average loss of 12 years of life per person who dies, based on what the real world numbers actually show. So, how could the authors of the article in PNAS get the numbers so wrong?
Well, there is one thing that they should certainly have done, which they didn’t do. They didn’t take co-morbid conditions in to account. An 82 year old with type 2 diabetes, heart failure, chronic obstructive pulmonary disease and high blood pressure has a much shorter life expectancy than an 82-year old without any underlying conditions.
And we know that most of the people who die of covid have multiple underlying conditions. According to official data from the US Centers for Disease Control (CDC), 94% of people who have so far died of covid in the US had at least one underlying condition, and the average person who died of covid had three underlying conditions. You would think that the authors of the article in PNAS would have taken this factor in to account, since the number of underlying conditions a person has makes a big difference to how much longer they can expect to live.
A separate study was published in Wellcome Open Research in April that did try to correct for co-morbidities. Somehow, even when factoring in co-morbidities, this study still managed to arrive at an average of 12 years of life lost per person dying of covid. In other words, factoring in co-morbidities made zero difference to the projected years of life lost. Very strange.
If that was correct, it would mean that the average person dying of covid in Sweden, being 84 years old, would have lived to 96 if covid hadn’t happened. That is in spite of the fact that this average person has multiple underlying co-morbidities, and also in spite of the fact that the average 84 year old in Sweden can only expect to live seven more years, and will on average die around the age of 91.
So, if the authors of the study are right, this would mean that the average person dying of covid is healthier than the average person, since the average person dying of covid has 12 years of life left, and the average 84-year old only has seven years of life left. But we know the exact opposite is true – the people dying of covid are in general significantly less healthy than the average person. Admittedly, the data used in the study are taken from Italy and the UK, and I’m extrapolating to Sweden, but I find it implausible that the difference could possibly be that big.
So, something is fishy about the numbers. What?
Actually multiple things.
First, the authors only include eleven specific co-morbidities in their analysis, which means that all other co-morbidities that could affect years of life lost are excluded. As an example, cystic fibrosis is excluded from the analysis. The average life expectancy of a person with cystic fibrosis is 44 years. If a 40 year old with cystic fibrosis catches covid and dies, they would be considered completely healthy in the modeling done in this study, and would contribute around 45 years of life lost, when their real life expectancy is much lower.
Obesity, widely recognized as the biggest risk factor for severe covid, is not included in the modeling (probably because the authors didn’t consider it a “co-morbidity”), which means that people with obesity are considered to have the same life expectancy as non-obese people. Ignoring risk factors in this way will give the impression that people who die of covid are healthier than they really are, which will in turn lead to an over-estimation of their remaining years of life.
Second, the severity of co-morbidities is not factored in. Someone with end-stage chronic obstructive pulmonary disease (COPD) has a much shorter life expectancy than someone with mild COPD, and is probably much more likely to die if they catch covid, but this was also ignored in the modeling.
So, although the modeling in this second study attempted to factor in co-morbidities, it did so in an incomplete way, which likely resulted in a big overestimation of the number of years of life lost.
In the sub-group analysis, where the authors divide things up by age and number of co-morbidities, they find that a person age 80+ with three co-morbidities likely loses 6-7 years of life if they die of covid. Considering that the average person dying of covid is 80+ and has three co-morbidities, this seems like a much more reasonable number than the twelve years presented above. But it still seems high when compared with the real world data we have at this point in the pandemic.
Let’s say this number is right though, and the average person who dies of covid loses 6-7 years of life. Considering that roughly 1,4 million people have now died of covid, that would mean around 9 million years of life have been lost to covid so far.
To gain some perspective on the issue, let’s talk about measles. Measles is a disease that mostly kills children under the age of five. So, whenever someone dies of measles, the average number of life years lost is around 80. As a result of the global obsession with covid this year, measles vaccination programs have been paused in 26 countries. That means 94 million children are at risk of not getting their measles vaccines. It will only take about 110,000 children dying of measles because they didn’t get their vaccine, for the total number of life years lost to be the same as those lost due to covid.
And measles is just one disease. There’s also polio, tetanus, and yellow fever, to name a few. These are diseases that maim and kill children, but which can easily be prevented with vaccinations. How many years of life will be lost in total due to lockdown and to the world’s single-minded focus on covid this year?
Probably many times more than are lost to covid directly.
You might also be interested in my article about the Swedish response to covid, or my article about whether or not long covid is really a new disease.
I am rolling out a ton of new science-backed content over the coming months, including:
- Analyses of the benefits and risks of all common supplements and medications
- The keys to a longer, healthier life (possibly quite different from what you may have heard)
- A long-term follow-up of the health consequences of the covid pandemic and global lockdown.
Please provide your e-mail address below and you will get all this content straight to your inbox the moment it is released.
Join 10,259 other subscribers
Email Address
Subscribe
The post How many years of life are lost to covid? appeared first on Sebastian Rushworth M.D..
NOT THE BABYLON BEE: Food deemed non-essential as New Mexico governor shuts down grocery stores.
HIGHER EDUCATION BUBBLE UPDATE: Harvard dismisses Title IX complaint against prof who said trans student would have been murdered in China. But wait, there’s more:
More surprising is that Harvard University didn’t punish a professor for stating that truth, even when it riled up a student who ranks high on the subjective oppression scale – though it took a month to clear him.
The Ivy League school dismissed a Title IX complaint filed against Arthur Kleinman (above) by a transgender student who claimed the anthropology professor created a “hostile environment” by noting how Kai De Jesus would be treated in “rural China,” The Harvard Crimson reports.
Kleinman insisted he was trying to stop De Jesus, a man who identifies as a woman, from derailing the virtual class session on the tradeoffs in global public health by suggesting violence against whites was justified.
Another student in the class, Shah Faesal, agreed that the transgender student’s question, in retrospect, appeared to justify the “extermination of the white race to bring an end to the race problem.”
It’s nice to know that our allegedly top universities are incubating “final solution” talk.
The post New Study Suggests That Surviving Coronavirus Gives You Long Term Immunity appeared first on The Bongino Report.
SHOCKER: Switching to e-cigarettes from smoking reduces toxic chemical exposure. “Switching to pod e-cigarettes significantly reduced exposure to toxins which cause disease, [and] smokers who made a complete switch experienced the greatest reduction in exposure, [while those] who made a partial switch also experienced reduced harm.” Obviously, we need to ban these immediately.
RUNNING AN “ELECTION” ON CLOSED-SOURCE VENEZUELAN VOTING SOFTWARE: That voting machine software in America is not open source and auditable is such a preposterously obvious security and hacking risk that the only reasonable conclusion is that it’s meant to be insecure and hackable. There is no commercial value in closed source voting software (it’s the machines themselves they’re selling; as software goes, it is trivial and nobody wants weird innovations or updates) unless part of the value proposition is that the vote can be rigged. The media and politicians can gaslight us all they want on this, but something this “stupid” doesn’t happen accidentally, even today and with our incompetent ruling class.
One of the most frequent questions I’ve been getting recently is how accurate I think the covid tests are, and in particular the PCR tests. As it happens, a systematic review has recently been published in Evidence Based Medicine that looks at the covid tests (both PCR and antibody), so I thought it would be interesting to look in to the evidence together. This article gets a bit technical and math-heavy in places, so please bear with me. I think the payoff is worth it.
First, let’s make sense of what the two types of test are and how they work. The PCR (Polymerase Chain Reaction) test is designed to detect a specific sequence of nucleotides, and when it comes to detecting SARS-CoV-2, the sample is usually taken from the back of the throat. Nucleotides are the building blocks of genomes, and the idea is that if you can detect a string of nucleotides that is specific for a certain organism, then that proves the organism is present at the sample site. Since PCR is designed to detect bits of viral genome that are currently present in your respiratory tract, its purpose is to detect a currently active infection (as opposed to a past infection).
PCR works by repeating a series of chemical reactions over and over. If the sequence of nucleotides that is sought is present in the sample, then each time the reaction is repeated, the number of copies of the sequence will double, so that more and more copies accrue.
So, if you start of with one copy of the nucleotide sequence you are looking for, then after one cycle you will have two copies. After two cycles you will have four copies. After three cycles, you will have eight copies. After four cycles, you will have 16 copies. And so on. As you can see, the fact that each cycle doubles the number of copies means that the numbers quickly build to massive levels. The covid PCR tests frequently keep going up to 40 (or sometimes even 45) times.
If you start off with just one copy of the viral nucleotide sequence in the sample, then after 40 doublings, you will have over 1,000,000,000,000 copies (that’s one thousand billion copies). The reason you do this repeated cycle of doubling, is that once you get enough copies of the sequence you’re looking for, then you can use other technologies to detect it. For example, you can add molecules to the sample that visibly light up if enough copies of the sequence are present. So after enough copies are present in the sample, then they can be detected, and you get a positive result.
The number of times you choose to cycle through the steps of PCR before you decide that there was no virus in the sample after all is known as the cycle threshold. The number of cycles used to get a positve result is actually a pretty important number, because it tells you how much virus is in the sample. The lower the number of cycles required, the more virus is in the sample. The higher the number of cycles, the more likely that the result is a false positive, caused perhaps by having a tiny amount of inactive virus in the respiratory tract, or by contamination of the sample in the lab. Like I said, after 40 cycles, even a single copy of the viral sequence has become over one thousand billion copies.
One thing that’s important to understand at this point is that PCR is only detecting sequences of the viral genome, it is not able to detect whole viral particles, so it is not able to tell you whether what you are finding is live virus, or just non-infectious fragments of viral genome. If you get a positive PCR test and you want to be sure that what you’re finding is a true positive, then you have to perform a viral culture. What this means is that you take the sample, add it to respiratory cells in a petri dish, and see if you can get those cells to start producing new virus particles. If they do, then you know you have a true positive result. For this reason, viral culture is considered the “gold standard” method for diagnosis of viral infections. However, this method is rarely used in clinical practice, which means that in reality, a diagnosis is often made based entirely on the PCR test. A systematic review looking at the ability to culture live virus after a positive PCR test found that the probability of a false positive result increased hugely with each additional cycle after 24 cycles. After 35 cycles, none of the studies included in that review was able to culture any live virus.
In most clinical settings (including the one I work in), all the doctor is provided with is a positive or negative result. No mention is made of the number of cycles used to produce the positive result. This is a problem, since it’s clear that a positive result after 40 cycles is almost certainly a false positive, while a positive result after 20 cycles is most likely a true positive. Without information about the number of cycles, you have to assume that the patient sitting in front of you has covid and is infectious, with all the downstream consequences that entails.
Anyway, enough about the PCR test for now. The other main type of test is the antibody test. Here, the sample is usually taken from the blood stream. There are five different types of antibodies, but most antibody tests only look for one type of antibody, IgG, which is the most common type. Generally it takes a week or two after a person has been infected before they start to produce IgG, and with covid, you’re generally only infectious for about a week after you start to have symptoms, so antibody tests are not designed to find active infections. Instead the purpose is to see if you have had an infection in the past.
One common method that is used for antibody tests is ELISA (enzyme linked immunosorbent assay). In this method, you have a plate on which you’ve fixed antigen that the antibody you are looking for can bind to (antibodies bind to antigens – antigen is short for “antibody generator”, and it’s basically the molecular structure that a certain antibody is specifically designed to bind to).
You then add the blood sample that you want to study to the plate, at which point the antibodies in the sample will bind to the antigens (assuming the antibodies you want to find are actually present in the sample). After that you wash the plate, so that any other antibodies in the sample that you’re not actively looking for are washed off (since there’s no antigen for them to bind to).
Next you add a signaling molecule that can bind to antibodies, and which has the ability to change color when exposed to a certain enzyme. You then wash the plate again. If there are no antibodies stuck to the plate for this molecule to bind to, it will wash off. If the antibodies you are looking for were present in the blood sample, they will have stuck to the antigen on the plate, and this new molecule will in turn have stuck to them.
Finally you add an enzyme that changes the color of the signaling molecule. If the signaling molecule hasn’t been washed off in the previous step, then you will see the plate change color, and the antibody test is positive.
Apart from understanding how the tests work, we also need to understand two important terms before we get in to the details of the recent systematic review. Those terms are sensitivity and specificity, and they are critical for all diagnostic tests used in medicine, because they tell you how good a test is.
Sensitivity is the probability that a disease will be detected if the person actually has the disease. So, for example, a test for breast cancer with a sensitivity of 90% will detect breast cancer 90% of the time. Nine out of ten patients with breast cancer will correctly be told that they have the disease. One out of ten will incorrectly be told that they don’t have the disease, even though they do.
Specificity is the opposite of sensitivity. It is the probability that a person who doesn’t have the disease will be told that they don’t have the disease. So, a specificity of 90% for our imaginary breast cancer test means that nine out of ten people who don’t have breast cancer will be correctly told that they don’t have it. One out of ten people who don’t have breast cancer will incorrectly be told that they do have it.
To put it another way, sensitivity is the ability of a test to detect true positives. Specificity is the ability of a test to avoid producing false positives. A perfect test will have a sensitivity and specificity of 100%, which would mean that it catches everyone who has the disease, and doesn’t tell anyone they have the disease if they don’t. No such test exists. In general, sensitivity and specificity are in conflict with each other – if you push one up, the other will go down.
If I just told everyone I meet that they have breast cancer, my sensitivity for detecting breast cancer would be 100%, because I wouldn’t miss a single case, but my specificity would be 0%, because every single person who doesn’t have breast cancer would be told that they do. So, when designing a test, you have to decide if you’re going to maximize sensitivity or specificity. If you design a covid PCR test with a cycle threshold of 40, then you are going for maximal sensitivity – the probability of missing a case is minimized, but you’re going to get a lot more false positives than if you set the threshold at 30.
Ok, now that we know what a PCR test is and what an antibody test is, and understand sensitivity and specificity, we can move on to the recent systematic review. The review included 38 studies of PCR tests (and LAMP tests, an alternative technique that is similar to PCR). The overall sensitivity for PCR/LAMP was between 75% and 100% in the different studies, while the overall specificity was between 88% and 100% . 16 studies, with a total of 3,818 patients, were able to be pooled together to get a more accurate estimate of sensitivity. In the pooled analysis, sensitivity was determined to be 88% . It wasn’t possible to determine a pooled specificity value, since the studies included in the pooled analysis were all of people who were already known with complete certainty to be infected with covid.
The review included 25 studies of antibody tests, but only ten of these (with a total of 757 patients) provided enough data to allow sensitivity to be calculated. The sensitivity of the antibody tests varied from 18% to 96%. 12 studies provided enough information for specificity to be determined, and in these it varied from 89% to 96% .
Ok, it might be hard to understand what these numbers mean in practical terms, so we’re going to play around with them a bit in order to clarify this, and I’m going to focus on the PCR test in this final discussion, since that is what’s generating much of the hysteria around covid. As mentioned, the sensitivity of the PCR test seems to be around 88% . A good value for the specificity is harder to determine, but it’s somewhere between 88% and 100%, so if we assume a specificity of 94% (halfway between the two values) we’re probably not far off.
Let’s say the disease is spreading rampantly through the population, and one in ten people are infected at the same time. If we test 1,000 people at random, that will mean 100 of those people actually have covid, while 900 don’t. Of the 100 who have covid, the test will successfully pick up 88. Of the 900 who don’t have covid, the test will correctly tell 846 that they don’t have it, but it will also tell 54 healthy people that they do have covid. So, in total 142 people out of 1,000 are told that they have covid. Of those 142 people, 62% actually have the disease, and 38% don’t.
That’s not great. Four in ten people getting a positive test result don’t actually have covid, even in a situation where the disease is so common that 10% of people being tested really do have the disease.
Unfortunately, it gets worse. let’s assume the disease is starting to wane, and now only one in a hundred people being tested actually has covid. If we test 1,000 people, that will mean ten will really have covid, while 990 won’t. Of the ten who have covid, nine will be correctly told that they have it. Of the 990 who don’t have it, 931 will be correctly told that they don’t have it, while 59 will be incorrectly told that they do have the disease. So, in total, 68 people will be told that they have covid. But only 9 out of 68 will actually have the disease. To put it another way, in a situation where only 1% of the population being tested has the disease, 87% of positive results will be false positives.
There is another thing about this that I think is worth paying attention to. When one in ten people being tested has the disease, you get 142 positive results per 1000 people tested. But when one in a hundred has the disease, you get 68 positive results. So, even though the actual prevalence of the disease has decreased by a factor of ten, the prevalence of PCR positive results has only decreased by half. So if you’re only looking at PCR results, and consider that to be an accurate reflection of how prevalent the disease is in the population, then you will be fooled, because the disease will seem to be much more prevalent than it is.
Let’s do one final thought experiment to illustrate this. Say the disease is now very rare, and only one in a thousand tested people actually has covid. If you test 1,000 people, you will get back 61 positive results. Of those, one will be a true positive, and 60 will be false positives. So, even though the prevalence of true disease has again decreased by a factor of ten, the number of positive results has only decreased slightly, from 68 to 61 (of which 60 are false positives!). So by looking just at positive PCR tests, you can easily be convinced that the disease is continuing to be roughly as prevalent in the population, even as it goes from being present in one in a hundred people to only being present in one in a thousand. The rarer the disease becomes in reality, the less likely you are to notice any difference in the number of tests returning positive results.
I want to restate this again, in a slightly different way, to make sure the message sinks in. As the disease drops enormously, by a factor of 100, from affecting one in ten to one in a thousand tested people, there is little more than a halving in PCR positive results, from 142 to 61. So a huge reduction in real infections only causes a small reduction in PCR confirmed “cases”. In fact, the disease could vanish from the face of the Earth, and you would still be getting 60 positive results for every 1,000 tests carried out!
The same trend is seen even if the PCR test were to have a much better specificity than we are estimating here, of say 99% . Here’s a quick illustration, since I don’t want to tire you with too many more numbers. If one in ten has the disease and you test 1,000 people, you will get back 97 positive results, of which 88 will be true positives and 9 will be false positives. If one in 100 has the disease, you will get back 19 positive results, of which 9 will be true positives and ten will be false positives. If one in 1,000 has the disease, you will get back 12 positive results, of which 11 will be false positives.
So, even if the test has a very high specificity of 99%, when the virus stops being present at pandemic levels in the population and starts to decrease to more endemic levels, you quickly get to a point where most positive results are false positives, and where the disease seems to be much more prevalent than it really is.
As you can see, the less prevalent the disease is in reality, the more likely the test is to generate a false positive result, and the less useful the test is as a method for figuring out who actually has covid. And the less prevalent the disease is, the more prevalent it will seem to be in relation to reality. If decisions about covid continue to be made largely based on what PCR tests show, we might never be able to call off the pandemic!
And that, ladies and gentlemen, is why PCR positive cases are a very poor indicator of how prevalent covid is in the population, and why we should instead be basing decisions on the rates of hospitalization, ICU admission, and death. If we just look at the PCR tests, we will continue to believe that the disease is widespread in the population indefinitely, even as it becomes less and less common in reality. And that is assuming the rate of testing doesn’t increase. If we combine this built-in problem with accuracy, with a massive increase in testing (as has happened in most countries over the course of the pandemic), then we can create the impression of a disease that is continuing to spread wildly through a population, even when it isn’t.
You might also be interested in my article about how deadly covid actually is, or, if you want to dig further in to the problems created by testing, you might be interested in my article about breast cancer screening.
I am rolling out a ton of new science-backed content over the coming months, including:
- Analyses of the benefits and risks of all common supplements and medications
- The keys to a longer, healthier life (possibly quite different from what you may have heard)
- A long-term follow-up of the health consequences of the covid pandemic and global lockdown.
Please provide your e-mail address below and you will get all this content straight to your inbox the moment it is released.
Join 8,084 other subscribers
Email Address
Subscribe
The post How accurate are the covid tests? appeared first on Sebastian Rushworth M.D..
One problem with all the trials of statins is that they look at the probability of still being alive after x years. But that’s not really the question patients want answered. Patients want to know how much longer they can expect to live if they take a statin every day for the rest of their lives. Is it weeks? months? years? decades?
Considering that statins do have known side effects, with muscle pain being the most common and widely recognized, and considering that many people think it’s annoying to have to take a pill every day, they generally want to know the size of the benefit before they decide whether to take the drug or not. Unfortunately, the answer to that question is hard to extrapolate from the studies, due to the way in which they have been designed. Saying that a drug decreases your risk of dying by x over five years doesn’t really tell you anything about how much longer you can actually expect to live.
In 2015, a group of researchers looked at the data from the statin trials and re-calculated the effect in terms of increased longevity. The study was published in the British Medical Journal, and it was funded by the University of Southern Denmark. One of the authors had significant conflicts of interest, having received money from multiple different pharmaceutical companies that produce statins.
All randomized trials comparing statins to placebo, and that also fulfilled the following three criteria, were included: They had to have at least 1,000 participants, they had to follow patients for at least two years, and they had to provide a survival curve. The reason a survival curve was necessary was because the increase in longevity was extrapolated by calculating the area between the survival curves for the statin group and the placebo group. I think the other two criteria are also reasonable – statin studies looking at mortality with less than 1,000 participants and that don’t even follow patients for two years are leaving too much up to chance.
The authors identified eleven studies that fulfilled the criteria, of which six were investigating statins for primary prevention (i.e. to treat people without known atherosclerotic disease) and five were investigating statins for secondary prevention (i.e. to treat people who had already had heart attacks, or in some other way clearly manifested atherosclerotic disease). These eleven studies together included a total of 92,135 patients, so the data are robust. Participants in the studies were followed for between two and six years. Most of the major statin trials (4S, WOSCOPS, ALLHAT, LIPID, ASCOT-LLA, JUPITER) were included in the analysis.
So what were the results?
Life was prolonged by between -5 and 19 days in the primary prevention trials (yes, that’s -5, as in minus five. In one of the studies people taking a statin lived five days shorter than people taking a placebo). In the secondary prevention trials life was prolonged by between -10 and 27 days (yes, again that’s -10, as in minus ten).
When everything is averaged out, people taking a statin for primary prevention lived three days longer than people in the placebo group. People taking a statin for secondary prevention lived four days longer than people in the placebo group. The average follow-up period in these studies was around four years, so if you assume that statins have a linear life-prolonging effect that grows with time (rather than petering off after a while, which is likely), then you can expect to live around one day longer for each year of treatment.
Huh? That’s disappointing. You take a drug dutifully, which your doctor has told you is vitally important, and it prolongs your life by mere days. The results are especially disappointing when you consider that most of the eleven trials were industry funded, and industry funded trials usually show better results than are seen in the real world. So most likely the real world benefit is even smaller than the tiny benefit found in these trials.
And remember, this analysis was done by people with financial ties to the pharmaceutical industry. If even people who are friendly with industry say that statins only prolong life by mere days, we can probably trust that the benefit really is that tiny.
As mentioned at the beginning of the article, statins are not completely free of side effects. So even if you are willing to take a drug every day that has an extremely marginal effect on longevity, then that benefit needs to be weighed against the risk of side effects.
You might also enjoy my article about whether statins save lives, or my article about whether the cholesterol hypothesis is dead.
I am rolling out a ton of new science-backed content over the coming months, including:
- Analyses of the benefits and risks of all common supplements and medications
- The keys to a longer, healthier life (possibly quite different from what you may have heard)
- A long-term follow-up of the health consequences of the covid pandemic and global lockdown.
Please provide your e-mail address below and you will get all this content straight to your inbox the moment it is released.
Join 8,632 other subscribers
Email Address
Subscribe
The post How much do statins prolong life? appeared first on Sebastian Rushworth M.D..
The post Flashback: (The Failing) New York Times Sounded Alarm on Dominion Voting Machines in 2018 appeared first on The Bongino Report.
A MESSAGE FROM OUR NEW ACTING SECRETARY OF DEFENSE: “Ending wars requires compromise and partnership. We met the challenge; we gave it our all. Now, it’s time to come home.”
Related: New Acting SecDef Is a Former ‘Horse Soldier’ Who Played Key Role in Afghanistan Invasion.
UPDATE: People seem unclear on what’s going on here, so here are my thoughts: There could be no victory in Afghanistan because the schwerpunkt of the Afghan conflict was Pakistan, since the Taliban are a creation of the Pakistani ISI. The U.S was unwilling to address Pakistan because it is a nuclear power, and a Saudi client. The schwerpunkt of the conflict with Pakistan, however, was Saudi Arabia, and Trump’s peace deal with the Saudis — which required them to stop supporting anti-US terrrorism — addressed that issue. But a Biden Administration will focus on reconciliation with Iran, and the Saudis will likely renege on the deal if (and when) they decide the U.S. has done so. The withdrawal from Afghanistan is an effort to get ahead of that, so as not to leave hostages, or to allow a more-obvious defeat.
FIGHTING TRUMP’S UNDERMINING OF OUR INSTITUTIONS BY undercutting civilian control of the military.

With press approval, natch.
I’LL TAKE TWEETS THAT DIDN’T AGE WELL FOR $500, ALEX:

I can’t wait for the explanation for this. Have Joy Reid’s time-traveling hackers struck again?
The post Joe Biden the Highest Recipient of Pfizer’s Political Donations in 2020 appeared first on The Bongino Report.
A very interesting article was recently published in Lancet that sought to understand which factors correlate, on a country level, with covid related outcomes. The study was observational, so it can only show correlation, not causation, but it can still give pretty strong hints as to which factors protect people from covid, and which factors increase the risk of being harmed.
The most interesting thing about the study, from my perspective, was that it sought to understand what effect lockdowns, border closures, and widespread testing have in terms of decreasing the number of covid deaths. Although correlation does not automatically imply causation, if there is a lack of correlation, then that strongly suggests a lack of causation, or at least, that any causative relationship that does exist is extremely weak. And considering the amount of money, effort, and resources that have been poured in to lockdowns this year, and that continue to be poured in to them right now, it would be pretty disappointing if lockdowns had such a minimal effect that there was no noticeable impact on mortality whatsoever. Am I right?
But I get ahead of myself. The study chose to limit itself to looking at the 50 countries with the most recorded cases of covid-19 as of the 1st of April 2020. My interpretation is that they chose the top 50 most affected countries, rather than looking at all 195 countries, due to resource constraints. Data was gathered up to the 1st of May 2020. All information gathered was in the form of publicly available facts and figures. Data gathered included information about covid, income level, gross domestic product, income disparity, longevity, BMI (Body Mass Index), smoking, population density, and a bunch of other things that the researchers thought might be interesting to look at. The authors received no outside funding and reported no conflicts of interest.
There are a few problems here that become apparent straight away. First of all, as mentioned, all the data in this study is observational, so no conclusions can be drawn about cause and effect.
Second, May was relatively early in the pandemic, and it’s now November, so we’re missing about half a year’s worth of covid data. On the other hand, the pandemic had already peaked in much of the world by May 1st, and lockdown measures had at that point been in place for months in most countries, so it should be possible to get a pretty good idea about what effect lockdown has in terms of decreasing covid deaths, even using only the data available up to May 1st.
Third, the analysis builds on publicly available data, often provided by different governments themselves, with widely varying levels of trustworthiness, and with different ways of classifying things. As an example, data from Sweden is infinitely more reliable than data from China. And while certain countries have used quite inclusive criteria when deciding whether someone has died of covid or not, other countries have been much more strict. The countries with stricter definitions will tend to have lower covid death rates than the countries with more generous definitions. This lack of homogeneity in how things are defined can make it harder to see real patterns.
Fourth, the reseachers who put this study together gathered an enormous amount of data, pretty much everything they could think of under the sun that might in some way correlate with covid statistics. That means that this study amounts to “data trawling”, in other words, going through every relationship imaginable without any a priori hypothesis in order to see which relationships end up being statistically significant. When you do this, you’re supposed to set stricter limits than you normally would for what you consider to be statistically significant results. They didn’t do this. We’re going to discuss this problem in more detail later in the article.
Before we get in to the results, I’ll just mention one more thing. The results are presented as relative risks (not absolute risks), which tends to make results look more impressive than they really are, and the statistical significance level is presented in the form of confidence intervals, not p-values (not a problem in itself, just a different way of presenting data). If you haven’t already done so, I strongly recommend you read my guide to scientific method before reading further, in order to make sure you understand all the terms used and gain maximal value from the content. Anyway, let’s look at the results.
The factors that most strongly predicted the number of people who died of covid in a country were rate of obesity, average age, and level of income disparity. Each percentage point increase in the rate of obesity resulted in a 12% increase in covid deaths. Each additional average year of age in the population increased covid deaths by 10% . On the opposite end of the spectrum, each point in the direction of greater equality on the gini-coefficient (a scale used to determine how evenly resources are distributed across a population) resulted in a 12% decrease in covid deaths. All these results were statistically significant.
Another factor that had an effect that was significant, but more weakly so, was smoking. Each percentage point increase in the number of smokers in a population was correlated with a 3% decrease in covid deaths.
Ok, let’s get to the most important thing, which the authors seem to have tried to hide, because they make so little mention of it. Lockdown and covid deaths. The authors found no correlation whatsoever between severity of lockdown and number of covid deaths. And they didn’t find any correlation between border closures and covid deaths either. And there was no correlation between mass testing and covid deaths either, for that matter. Basically, nothing that various world governments have done to combat covid seems to have had any effect whatsoever on the number of deaths.
We’re going to come back to this incredible fact in a little bit, but first we’re going to go off on a little tangent. As mentioned, the researchers didn’t correct for the fact that they were looking at a ton of different relationships, rather than just one single relationship between two variables. As I have discussed previously in my article on scientific method, the more relationships you look at, the more strictly you have to set the cut-off for statistical significance, since you will otherwise just by chance get a lot of relationships that seem significant but aren’t.
If you set a p-value of 0,05 (5% probability that a significant relationship was seen in a study even though there isn’t one in the real world), then one in twenty relationships you look at will be statistically significant just by chance. The 5% cut-off is intended to be used when looking at a single relationship, not when looking at multiple relationships. Now, in this study, the authors used confidence intervals instead of p-values, but that doesn’t change anything. A 95% confidence interval is equivalent to a p-value of 0,05, and so the same rules apply.
When you look at multiple relationships at the same time, you are supposed to correct for it. One way to correct is by using a method called the Bonferoni correction formula. This formula is very simple to understand. Say you have a p-value of 0,05 when looking at one relationship (the standard p-value in medical science). If you instead look at two relationships, you divide your p-value by two, thus getting a new p-value for significance of 0,025. If you are looking at ten relationships, you divide by ten, thus getting a new p-value of 0,005.
The authors who performed this study used a 95% confidence interval, as though they were only looking at one relationship between two variables. But they were in fact looking at a ton of variables (they never even specify how many) and a huge number of relationships, so they should have set their confidence interval much more widely.
They did have some results that they claimed were statistically significant, which I haven’t bothered to mention yet, because they’re certainly not significant after statistical correction.
For example, the authors claim a significant correlation between the Gross Domestic Product and covid deaths (relative risk 1,03, 95% confidence interval 1,00 to 1,06), and a significant correlation between the number of nurses per million population and covid deaths (relative risk 0,99, 95% confidence interval 0,99 to 1,00). But if you adjust, as they should have done, for looking at a large number of variables, then there is no way these results would still have been statistically significant. Sorry nurses.
So, what can we conclude from all this?
First of all, lockdowns do not seem to reduce the number of covid deaths in a country. Oops. Based on this data, if you want to decrease the number of covid deaths, you should encourage more people to start smoking, and possibly also start a communist revolution, to equalize wealth as far as possible.
Just kidding. As I’ve mentioned, the data is observational, so we can’t say anything about causality. What we can say from this is that lockdowns don’t seem to work – if they have any effect at all, it is too weak to be noticeable at a population level.
The other important finding from this study, from my perspective, is the strong link between obesity and risk of dying from covid. We can’t say that obesity in itself increases risk of dying – people who are obese have so many different biological systems malfunctioning at the same time that it’s impossible to say whether obesity is the cause of increased risk of death or just a marker of poor health in general.
Regardless, obesity is the strongest covid risk factor that we can do something about. And even if it isn’t the obesity itself that kills people, when we fix the obesity, we also fix the many derangements in metabolism and immune function that go along with it. So it is reasonable to think that efforts to decrease the rate of obesity in the population would decrease the number of people dying of covid. That is where we should be putting our efforts as a society right now – making people healthier so that their bodies are able to fight off covid (and cancer, and heart disease, and dementia, and all the other things that preferentially kill people with sub-optimal health).
You might also be interested in my article about whether vitamin D can be used to treat covid, or my article about whether a low fat or low carb diet is more effective for weight loss.
I am rolling out a ton of new science-backed content over the coming months, including:
- Analyses of the benefits and risks of all common supplements and medications
- The keys to a longer, healthier life (possibly quite different from what you may have heard)
- A long-term follow-up of the health consequences of the covid pandemic and global lockdown.
Please provide your e-mail address below and you will get all this content straight to your inbox the moment it is released.
Join 8,442 other subscribers
Email Address
Subscribe
The post Does lockdown prevent covid deaths? appeared first on Sebastian Rushworth M.D..


Two years ago, I was unsatisfied with my options for health insurance. The premiums were rising even as the quality dropped in the form of an ever-increasing deductible. I am guessing that you might feel the same way these days – most of us Americans are in the same boat.
I felt like I was being squeezed from both ends and it was starting to piss me off. So I decided to take some action, by doing the math for myself using a spreadsheet. I needed to answer the question, “Is this insurance really as bad a deal as I think it is?”
Sure enough, the risks and rewards of the coverage did not justify the premiums, so I decided to try an experiment and simply drop out of the market and insure myself. In other words, just rolling the dice and going through life with no form of health insurance at all.
Doubling down on the bikes, barbells and salads, I did my best to eliminate any risk factors that are in my control, while accepting that there are still much less likely but more random factors that are not.

Almost two years and $10,000 in premium savings later, I have found the experiment to be a success: I have slept well and not worried about the fact that I could be on the hook for a big bill if I did ever need major care. And as luck would have it, I also enjoyed the same good health as always over this time period – probably the best in my life so far because the extra healthy living has been working its magic.
But.
This situation has not been quite ideal, because my life is not a very useful model for everyone to follow. Most people don’t have the luck of perfect health, many have a larger family than I do, and very few people are in a financial position to self-insure for all possible medical bills.
Also, I found myself wishing I had a doctor that actually knew me, who I could call or visit on short notice if I ever did need help.
Finally, I wanted to switch back to having some form of insurance so that I could learn about it and write about it as time goes on. But was I really willing to be part of that unsatisfying and broken insurance model?
Then something magical happened: I learned about the new and vastly improved world of Direct Primary Care physicians.
What is DPC?
DPC is a fairly new trend in the US, but it is also a return to a very old tradition: a direct relationship between you and your doctor, with no insurance company in the way.
As a customer, you pay for a monthly subscription (somewhere around $100), and in exchange you get unlimited access to super elite, personalized medicine for the vast majority of your medical needs. Diagnoses, prescriptions, skin conditions, stitches, even fixing a broken bone if you don’t need surgery. All covered, with no co-pay and in an environment that feels to me like Presidential-level health care, in striking contrast to some of my past experiences where I felt like an anonymous numbered ticket in a sloshing sea of bureaucratic institutional medicine.
Oh, and direct email, phone and text message contact with your doctor, prescriptions over phone or video call, and in some cases even house calls depending on the practice and the situation.
Through some sort of magic, the Direct Primary Care model offers much better medical care and much lower prices, at the same time.
How could it be? It’s because of the incentives.
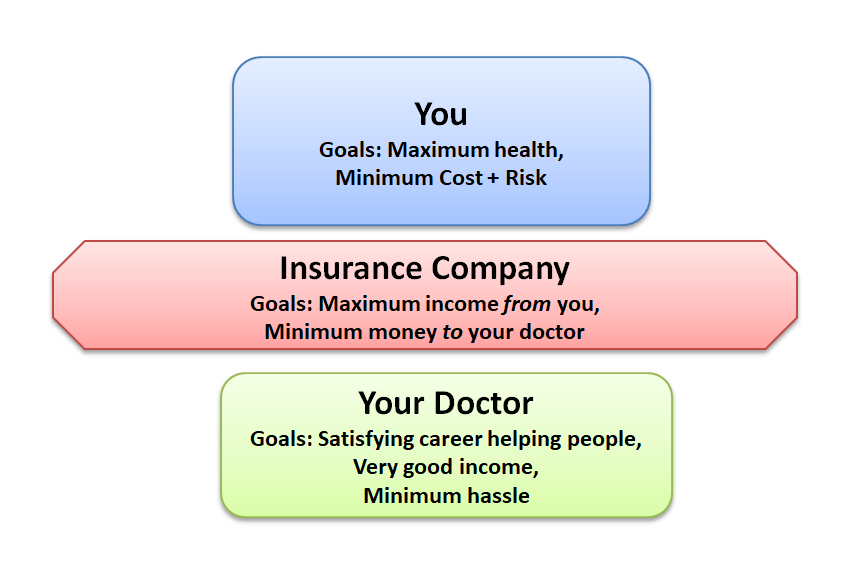
In our famously broken US healthcare model, an insurance company is wedged in between you and your doctors, and it has different objectives than you do.
You just want the best overall health for yourself, and when the shit does hit the fan and you need medical care, you want it to be quick, effective, and at minimum cost. And you don’t want to be hounded with years of stressful stray bills after an expensive medical procedure.
Your Doctor wants to help as many people as possible and make a good living, without having to wade through a sea of paperwork or stress or lawsuits.
Your Insurance company wants to make as much profit as possible, which means maximizing the amount they collect from you, and minimizing the amount they pay to your doctor. In theory, they benefit from helping you to stay healthy. But they have also developed elaborate contracts (putting in as many loopholes as possible to allow them to drop your coverage or deny claims), become masters of delaying payments, limiting which procedures and tests they will authorize doctors to do, and just generally throwing the biggest monkey wrench into the system that they can.
Over the decades, there has been a complex battle of lawmaking, lobbying, compromise and complexity to try to regulate away some of these problems. Sometimes the new laws help, sometimes they don’t, but the end result will never be optimal simply because there are a lot of people involved, and big crowds of humans make for slow and shitty decision making.
The Direct Primary Care Model

With DPC, it’s just you and your doctor. You both have the same incentives, but now the model works much better because there is no chaotic and expensive force in the middle to mess things up.
And because you operate on a subscription, the doctor gets paid whether you come into the office or not. At the same time, you are free to come in whenever you do need something, at no additional cost. So she has an incentive to keep you healthy, so that you have no need to come into the office in the first place.
On top of this, you get to decide together what is the best course of healthy prevention and treatment, without the overhead and complexity of constantly fighting with insurance companies. This drastically cuts the costs by eliminating the large staff of paper-pushers and attorneys that you normally need to operate a medical office, and frees up the doctor to spend more time with each patient during each visit.
How could the doctor possibly make a living with such low fees?
As it turns out, a small practice with one or two doctors and a few credentialed medical assistants can handle over 1000 subscribers while still giving each person much more time than they get under the old model. At $100 per month, this is $1.2 million in annual gross subscriber income, which is enough to pay everybody well, and rent a suitable clinic space. And as you scale up the operation, some economies of scale on things like space and equipment make it even better.
Just as importantly, running a practice like this tends to make a dramatic improvement in a doctor’s quality of life. It’s better medicine, with more flexibility and less hassle and stress. No wonder this model is growing rapidly and has become a favorite of physicians who happen to be MMM readers, as I hear from more of them every month.
Direct Primary Care is now a nationwide movement, with many hundreds of practices spanning the country and many more opening each year. Today’s screenshot of https://mapper.dpcfrontier.com/ shows the current state of the market.

In fact, it turns out this whole trend might even be a Mustachian-originated phenomenon, as I joined my own local practice called Cloud Medical, met the founder Dr. David Tusek, and he revealed halfway through our introductory visit that he was both a founder of DPC pioneer Nextera Healthcare in 2009, and a lurking reader of this blog for several years before I discovered him right here in my own town.
A note for locals: if you are considering joining Cloud, mention that you would like the MMM discount to save a further $12/month! (we have no affiliation, they are just looking to expand the practice and I’ll remove this notice if they fill up)
My experience (so far) with Cloud Medical
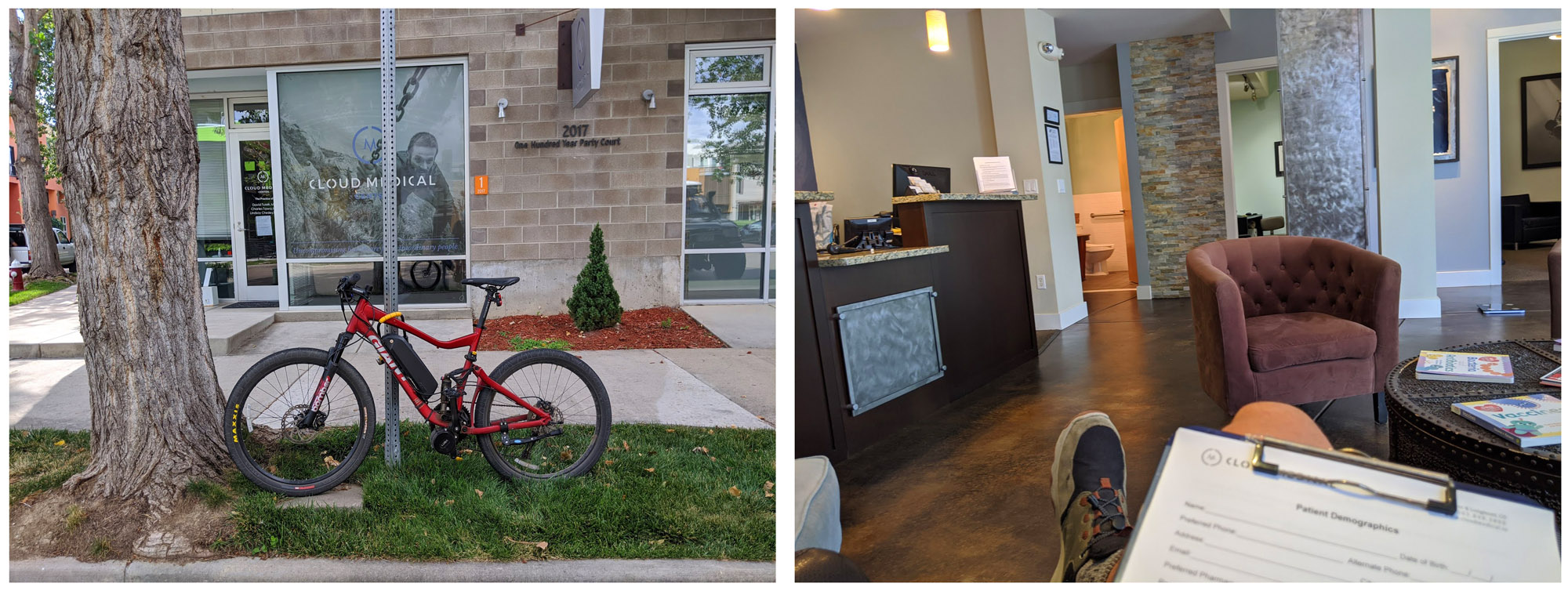
I signed up with Cloud this past summer, about five months ago. Although I have been feeling great, I figured it was time to put myself through an extensive battery of “middle-aged man” tests just to make sure I am not missing any hidden problems.
With the doctor’s guidance, I did a very thorough blood test, plus an electrocardiogram scan of my heart performance and ultrasound Carotid artery scan which involves a practitioner lubing up your neck and sliding a Star-Trek-style probe around on it while recording images of your body’s most critical plumbing to check for signs of clogging. Plus the usual checks of an annual physical exam. All clear.
I also finally got around to a long-awaited diagnosis and prescription for my Adult Attention Deficit Disorder condition, something which took me seven years to get organized enough to achieve, paradoxically one of the crippling effects of ADD. Although this is a very personal health detail, I mention it here because there are many friends and readers who also suffer from this condition, and I encourage you to learn more about it and seek help if appropriate. It can be life-changing. I found this process was much easier in a DPC environment, because of the more personal nature of the doctor-patient connection.
This DPC model addresses perhaps 90% of typical medical needs in-house, and a “menu” of optional specialists knocks out another 5%.

But there is still a chance you will need the more rare (and expensive) services of a hospital or specialist. In this case, your DPC physician can provide referrals and guidance to allow you to get the right help at a discounted, direct-pay price, or even handle your needs with a conventional insurance company.
Part Two: But What About Bigger Expenses?
At this point, you can add another layer of protection: High deductible conventional insurance, or a health share membership which offers a similar end-result while being careful not to be classified as insurance.
I think of health shares as a form of “emergency medical bill reimbursement”, rather than full fledged insurance. They are suitable for mostly-healthy people who want financial protection in the event of a major medical event. But they are not insurance, and often not too useful for someone with an existing, expensive condition.
Update 11/12: This blog post has triggered lots of fine-print-reading and discussion among readers, which led us to follow up with various insurance and health share companies.
The final word on one issue of debate: most conventional insurance and health shares do not cover voluntary abortions, while they do cover medically necessary ones, just under the different name of “Maternal Complications”.
Health shares in particular also don’t offer much ongoing drug reimbursement, which includes a lack of coverage for birth control. While I disagree with this policy, from a practical perspective it just means you need to budget for this expense separately.
For situations where a health share membership falls short, the subsidized and regulated insurance available through employer-based plans or the state exchanges via the Affordable Care Act, are probably a better bet.
But with all that in mind, I still chose one for myself, so let’s get into it!
Health sharing groups started out catering only to members of certain religions. Then a provider called Liberty Health Share opened up the market slightly while still requiring some fairly specific spiritual affirmations.
The latest incarnation is a company called Sedera* , which has addressed some of the shortcomings of earlier companies, has far less religious basis, and now seems to be the place that most of my more analytical friends and their families are ending up. Even my DPC physician Dr. Tusek is now recommending Sedera.
Sedera is worth a whole separate article in itself, and in fact I am starting a dedicated page for questions and answers and discussion on the experience. But for now, we’ll take a shortcut and just say that I was convinced and willing to give it a try, so I signed myself up as a Sedera customer.
A quick comparison of the closest standard insurance plan I could find on the standard Colorado health insurance exchange, versus what I got from Sedera (click for larger version):
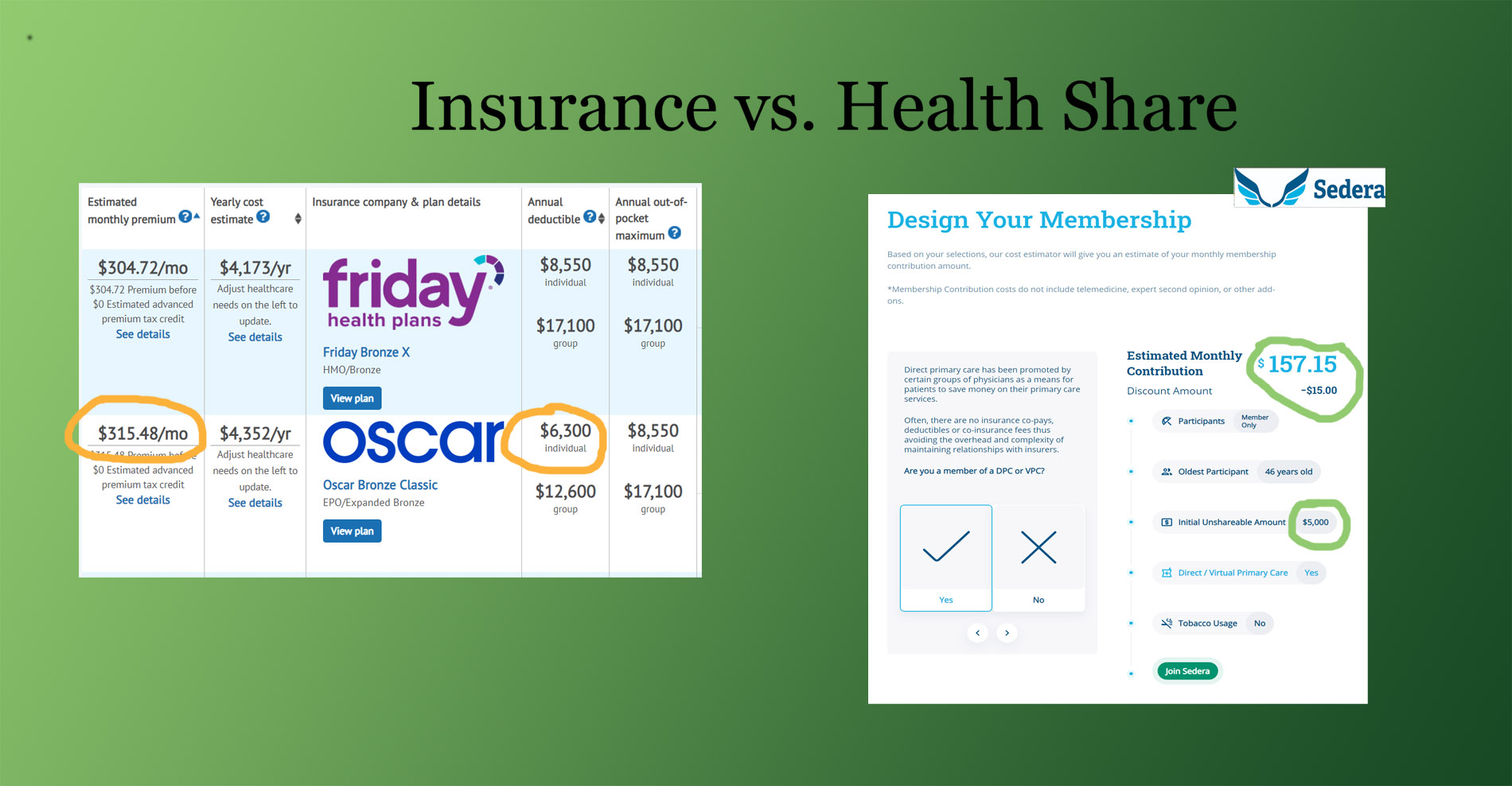
Another thing I like about all this is that there is no concept of “in network” and “out of network” doctors or hospitals. You can even use hospitals in other countries while traveling, and get reimbursed in US dollars after you return home. It’s simpler, cheaper and more flexible.
So in the end, by combining DPC with a health share membership, I am hopefully ending up with the best of all worlds:
This all sounds good to me, but it is important to state that this is an experiment. I still don’t have much experience with the US healthcare system – it helped deliver my son in 2006, and then repair that same boy’s broken arm in 2016. Conventional insurance offered some halfhearted support for both of those expenses, but aside from that I don’t have many stories to tell.
By collecting more information from readers and from my new helpers at Cloud Medical and Sedera, we should be able to make more sense of all this. And hopefully continue to expand and improve this new, better form of health care so it is accessible to more US residents.
If it gets big enough, we might end up solving this whole problem together – better, cheaper health care for everyone.
But What About the Affordable Care Act?
I think that DPC and ACA could work together perfectly – we keep the idea of the personal relationships, the subscription-based model, and the open and competitive pricing from hospitals for all procedures. But we just don’t need conventional insurance companies. If our society wants to help less-wealthy people to afford the best health care (which I think is a great idea), we could just subsidize their DPC memberships and offer a public insurance option at low or zero cost which covers hospitalizations. The reason this is better than the ACA: direct care and no insurance companies.
Conclusion
My past articles and experiences have shown that for many of us, a big hurdle when considering early retirement or self-employment is “what about health insurance”? Hopefully the is DPC + Healthshare method will put that question to rest for many of us. After all, shouldn’t our career and life choices be separate from our healthcare?
—–
Interested in Learning More?
A long-time friend of mine (and fellow early-retiree, and co-owner of the HQ coworking space) Bill and his family have been Sedera customers and enthusiasts for about two years. So much that he even took it upon himself to meet the company’s management, sign himself up as a representative to streamline some of the inefficiencies he perceived when joining, and then teach me about the whole thing.
Because of that, I am sharing Bill’s Sedera signup link in this article. His is unique among the Sedera affiliates in that he charges zero administrative fee, typical brokers charge $25 per month and up.
https:/sedera.community/thefireguild1
(Sedera also has an option with a different enrollment process for employers. If you run a business and you’re interested, send an email to info@thefireguild.com for more info.)
*note: Sedera does pay its affiliates a small referral fee for new customers, which does not affect your monthly bill – in fact, this link offers a lower price than subscribing directly through the company’s website. Thus, we believe this is the lowest cost way on the Internet to get this coverage.
As mentioned above, I’m giving Bill his own page to maintain on this site, where he can share his ongoing research and updates and answer questions: mrmoneymustache.com/sedera
***September 2022: Bill has just updated his page with new information***
Further Reading:
I was quite moved by this piece that Cloud Medical’s Dr. David Tusek wrote about “the ten heartbreaks” that led him to work since 2009 towards accelerating this better way to do healthcare.
An interesting story from Bill’s hometown, from a doctor who took this path way back in 2013:
South Portland Doctor Stops Accepting Insurance, Posts Prices Online
(from the Bangor Daily News)
I am more offended by how ham fisted, clumsy, and audacious the fraud to elect him is than the idea of Joe Biden being president. I think Joe Biden is a corrupt idiot, however, I think America would survive him like we’ve survived previous idiot administrations. However, what is potentially fatal for America is half the populace believing that their elections are hopelessly rigged and they’re eternally fucked. And now, however this shakes out in court, that’s exactly what half the country is going to think.
People are pissed off, and rightfully so.
Before I became a novelist I was an accountant. In auditing you look for red flags. That’s weird bits in the data that suggest something shifty is going on. You flag those weird things so you can delve into them further. One flag doesn’t necessarily mean there’s fraud. Weird things happen. A few flags mean stupidity or dishonesty. But a giant pile of red flags means that there’s bad shit going on and people should be in jail.
Except for in politics, where apparently all you have to do to dismiss a bunch of red flag is be a democrat and mumble something about “fascist voter suppression” then you can do all sorts of blatant crime and get off.
I’ve been trying to keep up with the firehose of information about what’s going on during this clusterfuck of an election. Last night I was on Facebook talking about the crazy high, 3rd world dictatorship level voter turnout levels in the deep blue areas of these swing states was very suspicious. Somebody gas lighted me about how “I’d have to do better than that”, so this was my quick reply, listing off the questionable bullshit I could think of off the top of my head:
The massive turn out alone is a red flag.
But as for doing better…
The late night spikes that were enough to close all the Trump leads are a red flag.
The statistically impossible breakdown of the ratios of these vote dumps is a red flag.
The ratios of these dumps being far better than the percentages in the bluest of blue cities, even though the historical data does not match, red flag.
The ratios of these vote dumps favoring Biden more in these few battlegrounds than the ratio for the rest of the country (even the bluest of the blue) red flag.
Biden outperforming Obama among these few urban vote dumps, even though Trump picked up points in every demographic group in the rest of the country, red flag.
The poll observers being removed. Red flag.
The counters cheering as GOP observers are removed, red flag.
The fact that the dem observers outnumber the GOP observers 3 to 1, red flag (and basis of the first lawsuit filed)
The electioneering at the polls (on video), red flag.
The willful violation of the court order requiring the separation of ballots by type, red flag.
USPS whistleblower reporting to the Inspector General that today they were ordered to backdate ballots to yesterday, red flag.
The video of 2 AM deliveries of what appear to be boxes of ballots with no chain of custody or other observers right before the late night miracle spikes, red flag.
Any of those things would be enough to trigger an audit in the normal world. This many flags and I’d be giggling in anticipation of catching some thieves.
And it isn’t that I have to do better. I’m just an gen pop observer who happens to be a retired auditor with a finely tuned bullshit detector. This is going to the courts.
##
So now I want to delve into some of these some more. The problem is that there’s a ton of info swirling around, some good, some crap. It doesn’t help that reporters are usually dishonest or not very bright and absolute trash at presenting data. Part of our problem is Big Tech is actively stomping on stories that make their guy look bad. (while compiling these I discovered that several of the links I’d looked at yesterday had been vanished by Facebook or Twitter)
For the last four years half the country was all “Trump is illegitimate! He’s not my president! He stole the election!” so on and so forth, and that was all based upon nebulous ideas about “Russian Interference”, The Russian Interference mostly boiled down to them buying ads on Facebook, or having fake bots trolling on Twitter last time. This time the actual giant megacorporations, Facebook, Twitter, and Google themselves have actively censored stories in order to protect their candidate. So you think after this pile of suspicious election clusterfucks that makes the game look totally rigged, the other half of the country is going to accept Joe Biden as legitimate? Oh hell no.
When you are auditing you see mistakes happen all the time. Humans make errors. Except in real life, mistakes usually go in different directions. When all the mistakes go in the same direction and benefit the same parties, they probably aren’t mistakes. They’re malfeasance.
Let’s go back a bit to before election day to see why people would be suspicious that the game has been rigged.
Most of the mainstream polls were utter garbage, off by what I believe to be the largest amounts ever in all of American history. Of course, this thing that surely demoralized the right and helped the left raise funds was just an innocent sampling error rather than a purposeful sampling bias… uh huh.
Then in the weeks leading up to the election, Big Tech and the media had a concentrated censorship effort to stop what was probably the juiciest October Surprise in modern history. But them silencing major newspapers and US Senators was just a mistake in their innocent efforts to “fact check”.
Then on election day, states like Florida that were obviously swinging hard for Trump with no possible mathematical way for Biden to come back, the news wouldn’t call for Trump. States where it was still clearly up in the air just based on even the most cursory of statistical analysis (Arizona) they called for Biden ASAP. But that was just innocent mistakes, and not an attempt to set the narrative of inevitable Biden victory by major media.
When Trump pulled ahead in the midwestern swing states by what were starting to appear to be insurmountable amounts, they suddenly threw the brakes on the counts. (my favorite part of this was when it looked like Trump was going to win, the Chinese Yaun crashed, which is pretty telling about just how shitty a candidate Joe Biden is) Okay, suddenly stopping all those counts seemed a little weird, but most of America went to bed thinking that this was a close race, with Trump in the lead in the EC.
Then we woke up in the morning, and everybody saw the 538 graphs showing a massive middle of the night spike for Joe Biden, with almost zilch in corresponding votes for Trump.
Now, one of those got walked back as “typo”. (again, funny how all these “mistakes” keep going in one direction) but the damage was already done, and all of a sudden most of America was paying a whole lot more attention to places like Wisconsin and Michigan than we usually do. That’s how flags work. And it turned out that single six figure typo was only one of many statistically improbable Biden vote dumps to come.
Now, all of my liberal acquaintances were quick to dismiss these, with some gas lighting about how it was just deep blue inner cities votes coming in, and of obviously they’re going to vote for Joe Biden… Except that is them deliberately missing the point. It isn’t that Biden won those, it is that he won them with statistically improbable amounts.
I don’t know what the current numbers are now, but as of yesterday morning the Wisconsin Midnight Mystery Dump was something like 98.4% for Joe Biden. That’s better than the bluest of blue cities manage. That’s better than Biden did in DC. I saw one 28k dump yesterday (I want to say it was 538 talking about PA) that was listed as ALL for Biden. That’s basically statistically impossible.
In a small populace, you can get 100% of the vote. However the larger the sample, the more likely there will be dissenting votes. Even in the bluest of blue areas or reddest of red areas, somebody is going to be a cranky dissident, or an old person is going to fill in the wrong circle. When you get into the hundreds or thousands yet maintain that kind of perfect ratio, basically impossible.
Plus we are supposed to believe that Joe Biden, the guy barely campaigned, who got like 12 sad looking people to his rallies, was more popular than Hillary Clinton or Barack Obama? This election was just that much more special? Uh huh… Except that these few battleground state blue cities vote ratios don’t match up with other blue cities around America, where it appears Trump’s support among every demographic group other than white males went UP.
Then people were quick to dismiss these statistically improbable spikes with “of course the mail in voting favors Biden, republicans vote in person.” Yes, but they don’t favor Biden with these kind of ratios anywhere else in America. The ratios are more like 60-40 or 70-30. But 97-3? Oh fuck no. So either Biden is a better campaigner to the inner cities (though he rarely left his basement) than the eloquent messianic figure of Barack Obama, or there’s something fishy going on here.
Now, as a suspicious auditor type who spent a lot of hours looking for fuckery in complex systems, my gut tells me fake ballots were getting dumped into the system to make up the difference. And oh look, here is a giant pile of red flags indicating that’s the case.
Yesterday there was a meme going around about how Wisconsin
had something like 90% voter turnout, and how this was 20 points higher than
usual, and it how it would also be one of the highest voter turnouts in all of
American history. If Wisconsin was at 90% that beats the highest national number
in all of American history by EIGHT points. And that was 1876 (which was legendarily
fraudulent by the way).
Except, this is the problem with using memes to make your argument, it was only
partially accurate, and the previous Wisconsin numbers were cited one way, and
the current year was calculated a different way. (don’t feel bad, I fell for that
one too, and as an accountant, that’s SO ANNOYING). When most people think of
voter turnout, they think what percent of registered voters vote. But because
Wisconsin has same day voting (a gift for fraudsters) their prior year percentages
were votes compared to eligible population (that’s so goofy). But it meant the
meme was comparing apples to oranges. So the leftists immediately jumped on
that error to dismiss the idea that there was anything weird about how many
people turned out to vote this time.
HOWEVER, that’s useless obfuscation. Because if you calculate the number the same way that most Americans do, their turn out was still like 90%, which is a rate normally reserved for dictators (that combined with the vote ratios would have made Saddam Hussein blush). I had one liberal guy point out that notoriously corrupt Seattle also gets 90%… which doesn’t exactly help his case.
Because here’s the kicker, the high turn out is the average
for the state, but when you drill down on the source of these statistically
improbable blue vote dumps, they’ve got districts with TWO HUNDRED PERCENT TURN
OUT. That’s over 200%. There’s 7 over 100%, and a ton of them in the 90s. https://mkecitywire.com/stories/564495243-analysis-seven-milwaukee-wards-report-more-2020-presidential-votes-than-registered-voters-biden-nets-146k-votes-in-city
Now the quick liberal dismiss explanation for this is that Wisconsin has same
day registration (again, a fraudsters dream) and thousands of people ignored
months of TV and social media beating them over the head to get registered to
vote, and just decided to do it at the last minute because Biden is just that
awesome/Trump is just that bad.
Except if you’re an auditor, when you see super suspicious spikes like that in certain places, the first thing we think is that’s the place where you’ve got somebody over the controls colluding. So that’s where you go to fabricate your bullshit.
200% turn out is fucking insane. Same day voting or not. That’s madness. When I was looking into this stuff I pulled a HuffPo article about the 2012 election and how it was controversial that some Madison ward had gotten 119% turnout.
Oh, but wait, there’s more.
A whistleblower has come forward from a Michigan post office saying that they were given ballots on November 4th, and ordered to post mark them to election day so they would still be valid. https://www.facebook.com/JamesOKeefeAuthor/videos/381073273044980
That is so insanely illegal. When the reporter called the postal supervisor who gave the order and asked about it, he immediately hung up.
Now, on this one, liberals were quick to dismiss it because it was from Project Veritas. (who they hate, and say cherry picks their investigative reporting, yet they keep winning all the lawsuits against them) However, the very next video was the response from the US Postal Inspector General (or whatever his title is, I can’t remember) about how they are investigating, so this wasn’t just some crank going to a reporter, it’s been passed up the chain of command. It’s an actual whistle blower.
I had someone else try to dismiss this one as innocent, because the post office accepting these late ballots had no way of knowing who they voted for so it would balance out. That’s is so naïve its cute. Of course they knew who the ballots were for. They were probably dropped off by people they were colluding with. You don’t commit felonies for clueless strangers because you feel sorry they got their votes in late.
A quick note on collusion because I mentioned it a couple times now. Collusion is the key to successful fraud. Systems have controls and checks in places, so the best way to circumvent them is to team up with somebody over one of those controls and exploit the gap. That’s fraud 101. Which is why you go to the post office your buddy runs to drop off your illegal late emergency Save Biden ballots. Or you go to the ward your buddy the poll worker is running the log in book to same day register all your imaginary friends.
Speaking of the imaginary vote, this one is actually hilarious. Democrats are quick to say all votes must count, which apparently includes people who are 118 years old. https://twitter.com/fleccas/status/1324216584219623424?s=21&fbclid=IwAR2rMt9iguDDYq_6H1FTQtMGekNEiTRRUNVsXN9xiEGvxS8z2VhHLJwo6-s
All those little fraud schemes come in from various
directions, except the fraud numbers add up quick in a tight race. However, if
you are behind by hundreds of thousands of votes in the middle of the night it
requires some audacious level fuckery, which brings us to a red flag you can
see from space. The 4 AM Biden Miracle. Here is an account from somebody at the
counting center. https://www.facebook.com/iamconniejohnson/videos/10225096326823289
This is the third link I’ve had to pull for this one, because Facebook keeps
killing the others. Listen to the whole thing. Because after the statistically
impossible votes came in, they had to toss a bunch of the GOP judges out of the
building because of Covid.
Remember what I said about collusion? If you’ve got the actual system with the controls on your side, you can basically do any outlandish bullshit you feel like, and the only way you are going to get stopped is by an outside power (hence the multitude of lawsuits we’re going to see over the next few days).
Another thing you learn to spot when people are fraudulently manipulating data, is the mission-oriented spikes. On this one I’ve seen a few links, but the data has been so in flux that I’ve not been able to confirm it, but supposedly a bunch of the sudden Biden spikes weren’t just statistically improbable, they also voted for president but not the down ballot races. Now, lots of people will vote for president but don’t care about down ballot. However, when you get a pile of those in a row, that suggests somebody in a hurry filling out the mission critical bubble and then moving down stack, assembly line style.
There was also video taken of one guy delivering these mystery ballots to the counting center in the middle of the night (unloading them from a white van into a little red wagon) the link I used yesterday had been deleted by YouTube but I found this new one (can’t stop the signal, Mal) https://www.youtube.com/watch?v=Yh7h3w75D8U&feature=youtu.be
Gee whiz. I can’t imagine why mysterious boxes are being moved into this supposedly secure voting facility in the middle of the night with no observers or chain of custody.
And there’s more. They just keep coming. Yesterday morning I saw a small article about a republican official calling shenanigans on the voting in his small county, which went overwhelmingly Trump last time, and how it appeared the votes tallied weren’t even enough to account for his immediate family. Of course he got laughed at by caring liberals. Fast forward a few hours and it turns out that the voting program was faulty. https://www.westernjournal.com/election-program-issue-tallied-2-votes-gop-candidate-33-mi-counties-thought-using-software/
Worse, the same broken ass software was apparently used in 33 other counties. Hmmm… Again, with all these magical errors in these swing states all going in one side’s favor.
Then there’s SharpieGate, but I’ve heard so much conflicting stuff about that one, with sharpies actually working fine in the scantron machines, that I’m not putting much stock in that one yet. There’s a lawsuit already though, so it’ll be interesting to see what new information comes out.
Here’s another thing you learn about auditing. The more chaotic the system, the more chances for fraud. So when you come across a system that is extra chaotic on purpose, that tells you that the people running it want it that way for a reason.
And the flags just keep coming in. This is going to be way worse than Florida in 2000.
What happens now? Beats me. It goes to court, and then the real question becomes how much spine the republicans have to actually fight. In previous years I’d assume they’d be a bunch of spineless chickenshits and wimp out like usual, but I’m not so sure this time. I don’t know if or how any of these will pan out, and without access to the real data, all I can do is guess.
I can say without hesitation though, that fuckery is afoot, and if an actual real investigation happens they’ll be able to prove it. Only this is politics, so who knows. The only thing I do know for certain is that this election is so fucked up it is just going to make America’s two halves hate each other even more.
Update: I did a part 2 https://monsterhunternation.com/2020/11/09/election-2020-the-more-fuckery-update/

Michigan voters Tuesday night had a message for police: Get a warrant. Yes, for their phones, too.
Voters overwhelmingly approved Michigan Proposal 2. The referendum, put to the ballot by lawmakers, amends the state constitution to add "electronic data and electronic communications" to the state's search and seizure laws.
With 88 percent of the vote counted, Michigan voters approved the protections. The measure passed with 88 percent of the vote, more than 3.8 million votes of support.
The relevant part of the state's constitution will now read:
The person, houses, papers, possessions, and electronic data and electronic communications of every person shall be secure from unreasonable searches and seizures. No warrant to search any place or to seize any person or things or to access electronic data or electronic communications shall issue without describing them, nor without probable cause, supported by oath or affirmation. The provisions of this section shall not be construed to bar from evidence in any criminal proceeding any narcotic drug, firearm, bomb, explosive or any other dangerous weapon, seized by a peace officer outside the curtilage of any dwelling house in this state.
Ballotpedia notes that the changes passed unanimously through both Michigan's House and Senate in June before being sent to voters for approval.
It's another nice little reminder that there were a lot of liberty-minded ballot initiatives that did very well last night that shouldn't be ignored as so many people obsess over who will control the White House and Congress.
The post Dems Are Trying To Steal The Election In Michigan, Wisconsin, And Pennsylvania appeared first on The Bongino Report.
DISPATCHES FROM THE EDUCATION APOCALYPSE: 65% of College Students Say Rioting and Looting is ‘Justified,’ New Poll Finds.
VITAMIN D UPDATE: More than 80 per cent of hospitalized COVID-19 patients had vitamin D deficiency. “For the study, the 216 hospitalized patients’ vitamin D levels were compared to those of a control group of 197 people of similar age and sex from a population-based cohort in the same geographical area. . . . The study’s authors were particularly interested in studying vitamin D because they said there’s evidence to suggest it plays a role in COVID-19 infection. Vitamin D is a hormone produced by the kidneys, which controls blood calcium concentration and affects the function of the immune system. Vitamin D deficiency has also been linked to health concerns including heart disease, diabetes, cancer, and multiple sclerosis. According to the study, there is also ‘compelling evidence’ for an epidemiological association between low levels of vitamin D and infections such as influenza, HIV, and the hepatitis C virus.”
THIS IS WHAT CAUSES ME TO WAKE UP SCREAMING: Joe Biden Inadvertently Tells the Truth.