by Bryan Menegus on Sploid, shared by Cheryl Eddy to io9
Australia is best known for animals that are needlessly good at murdering things. The country is also home to the tawny frogmouth, an incredibly stupid looking bird.
by Jennifer Ouellette on Gizmodo, shared by Cheryl Eddy to io9
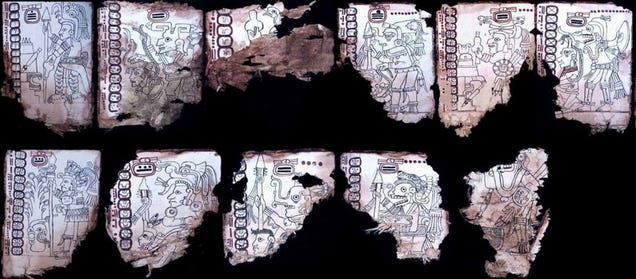
Scientists have been arguing over the authenticity of an ancient document called the Grolier Codex for 50 years. A new analysis published in a special section of the journal Maya Archaeology has concluded that the codex is indeed genuine, making it the oldest surviving manuscript from the pre-Colombian era.
Yet, I suspect these kinds of situations are relatively rare. Having been involved in enough papers, and, yes, being party to papers where I didn’t catch something in the review or editorial process, I have the ultimate answer:
Reviewers, editors, and authors are human.
What I mean by this is that scientific papers are complex beasts. A single manuscript may weave together disparate groups of organisms, unfamiliar pieces of anatomy, far-flung reaches of the globe, and multiple statistical techniques. A typical paper is usually seen by a single editor and two to four reviewers. It is extremely unlikely that every facet of the paper will be seen by an appropriate expert on that given facet. How likely is it that every error will be caught and addressed?
Philippine President Rodrigo Duterte has taken his “bad manners” – having gained global notoriety with his election campaign insults earlier this year – to a new level.
If that were all there was to it, we could rightly roll our eyes and move on. After all, Duterte’s language is vulgar; his slander of people and groups is liable to incite violence; and his determination to kill drug pushers (to fight “crime with crime”) an abuse of power. He should not be defended for any of this.
But as someone who has spent a long time studying US-Philippine relations, I think there’s something more for us to see here. And if we want to judge the Philippine president (and, by default, the nation for electing him) from high moral ground, I think we have a responsibility to pay attention to it.
Restoring an invisible history
Who is he to question me about human rights and extrajudicial killings?
So asked Duterte on Monday. It’s actually a very good question, and one long overdue from a Philippine president. The extent to which the violence of US relations with the Philippines has been made invisible by a history written predominantly by Americans themselves cannot be overstated.
It began with a three-year war (1899-1902) that most Americans have never heard of. The war overthrew a newly independent Philippine republic and cost between 250,000 and a million Filipino lives – only to be called “a great misunderstanding” by American colonial writers.
After all, the US had chosen the Philippines to be its great Asian “showcase of democracy”. The invasion was a benevolent act. Hence the complete erasure of acts of American violence from the Philippine national story.
The 20th Kansas Volunteers march through Caloocan after the battle of February 10, 1899, early in the war that toppled the first Philippine republic.
G.W. Peters/Internet Archive
You don’t need to be a conspiracy theorist to smell something rotten. Since the 1950s Philippine writers, academics, journalists and so on have been trying to reframe the historical narrative to point out this fact: to be invaded by a military power, told you don’t possess the character or capability for self-government, and then controlled by another nation for four decades, to the occupier’s lucrative commercial benefit, was not to be the recipient of a benevolent act.
Even at the time the war was taking place, one of America’s best-loved authors was writing just as much. Mark Twain was prolific in writing about the paradox of the “democratising mission” to the Philippines.
The Person Sitting in Darkness is almost sure to say: ‘There is something curious about this – curious and unaccountable. There must be two Americas: one that sets the captive free, and one that takes a once-captive’s new freedom away from him, and picks a quarrel with him with nothing to found it on; then kills him to get his land.'
In America, these remain Twain’s least-known works.
Before his (now regretted) distasteful remark, Duterte had much to say in response to the question about being confronted over human rights in an upcoming meeting with Obama. He was responding to murmurs from critics that, if he wouldn’t listen to anyone else about the extrajudicial killings in the Philippines, just wait until he meets the US president.
No-one seems to have listened to or cared much about the other six minutes of Duterte’s reply. So let me tell you something about it. It was a reclaiming of the historical narrative of Philippine-US relations, a holding up to the US of the hidden “looking glass” Mark Twain had written about 100 years earlier.
The Macabebe Scouts were a native Filipino force of the US Army during the Spanish–American War.
The Ardvaark/Wikipedia Commons
An assertion of independence
Calling out the hidden insinuations, as Duterte did, that the US continues to have authority over the politics of the Philippines, is bold and brazen, but reasonable. Consider his statement:
I am a president of a sovereign state. And we have long ceased to be a colony. I do not have any master but the Filipino people.
These words are less evidence of his demagoguery or an intention to personally disparage Obama than a reference to history, and are more accurately read as such.
After the second world war, colonies of any sort, even the so-called “democratic” US one in the Philippines, were on the nose. But this didn’t stop Washington officialdom from continuing to claim the right of access to the Philippines' political and economic realms.
When the US finally granted the Philippines its (second) independence in 1946, it required the new republic to amend its constitution so a bill could be passed that, as well as legislating preferential trade conditions for the US, would grant American citizens equal rights with Filipinos to Philippine natural resources. It was the beginning of a new phase: neocolonialism.
It was not just a matter of political interference and the power to make or break Philippine presidents with endorsement and strategic financial support. In a visceral sense, the nation was always being watched and judged by its democratic “teacher”.
School Begins: Uncle Sam lectures his class in Civilisation (the pupils are labelled Philippines, Hawaii, Puerto Rico and Cuba).
Puck Magazine 1899
Asked about being confronted with human rights concerns by Obama, Duterte said:
You must be kidding. Who is he to confront me? America has one too many to answer for the misdeeds in this country … As a matter of fact, we inherited this problem from the United States. Why? Because they invaded this country and made us their subjugated people … Can I explain the extrajudicial killing? Can they explain the 600,000 Moro massacred in this island [Mindanao]? Do you want to see the pictures? Maybe you ask him. And make it public.
I’m reminded of a comment by Alicia Garza, a founder of the Black Lives Matter movement ignited by police killings of black Americans. Speaking in Sydney last weekend at the Festival of Dangerous Ideas, she related how, when civil rights protests get uncomfortably heated, she is often asked: “Why are they so angry?” She paused. Then softly giggled, giving the audience time for the ludicrousness of the question to sink in.
Why is the Philippines president so angry about the prospect of the US president confronting him about human rights abuses? History. As Duterte said himself on Monday, violent acts of the past don’t stay in the past. They get passed on from generation to generation, especially when the injustice goes unacknowledged and unaddressed.
It is difficult to stomach Duterte’s style. It certainly is difficult to look past the serious issues raised by his administration’s “war on drugs”. We should condemn his misuse of power.
But if we condemn the president for his recent remarks because we claim to be concerned about the rights of Filipinos while showing no interest in acknowledging the past crimes and injustices against the Philippines, we fall into our own sort of hypocrisy.
Let’s be honest, if Duterte didn’t curse and swear and offend our sensibilities, would we be paying so much attention to the Philippines? For once, I heard a Philippine president holding the US to account for all its doublespeak and hypocrisy in US-Philippine relations. And I couldn’t help but appreciate that.
Adele Webb does not work for, consult, own shares in or receive funding from any company or organization that would benefit from this article, and has disclosed no relevant affiliations beyond the academic appointment above.
by Terry Slevin, Adjunct Professor, School of Psychology and Speech Pathology, Curtin University; Education and Research Director, Cancer Council WA; Chair, Occupational and Environmental Cancer Committee, Cancer Council Australia
A report this week from the Australian government’s National Industrial Chemical’s Notification and Assessment Scheme (NICNAS) shows what’s in the ink that’s under the skin of more than 2 million Australians and about 100 million Europeans. And it’s not pretty.
The report found 471 different tattoo inks likely to be used in Australia made up of 89 unique chemicals. They interviewed 22 professional tattoo artists and sourced 49 specific tattoo inks likely to be used in Australian tattoo parlours for detailed chemical analysis.
Of the 49 inks NICNAS tested, only four complied with the European standards.
The major concern was the presence of polycyclic aromatic hydrocarbons (PAHs), a group of chemicals known to be carcinogens. PAHs were found in more than one-fifth of the samples tested and in 83% of the black inks tested.
Other non-compliant components include barium, copper, mercury, amines and various colourants.
In some inks, there was a mismatch between the content and the labelling.
One ink was sold and used for tattooing when the container label said it was not intended for this purpose.
Gone are the days of tattoos being seen only on bikies and sailors. Increasing proportions of the population have increasing proportions of the dermal layer of their skin injected with the multi-coloured artworks. There is no sign of demand dropping off.
This is an international challenge for regulators. Italy, for instance, had an eight-fold increase in the number of tattoo parlours from 2006 to 2015. Like us, they struggle to monitor what the effects might be.
Swiss health authorities analysed 416 ink samples and found 39 colourants that were never tested for use in contact with the human body.
Traditional Maori tattoos (moko) are a treasure protected by the Treaty of Waitangi, so regulation in New Zealand has special challenges.
It’s important to remember that humans have been tattooing their skin for thousands of years using various methods, some very crude. Outside the risks of infection from unclean injecting equipment, and some serious pre-existing medical conditions, there is little evidence directly linking tattooing to serious illness.
However, a German study found 67% of tattooed people reported complications. Of those, 7% were systemic (affecting more than just the skin around the tattoo) and 6% were persistent. These are mostly superficial skin infections but have included bacterial infections such as staphlococci and streptococci, mycobacteria and, in some rare cases, blood-borne viruses such as hepatitis B and C.
So what does all this mean? In short, no one really knows. Will everyone with ink get cancer? No. But the basics of toxicology tell us that the harm any substance does is influenced by how “poisonous” the substance is, the circumstances and nature of the exposure, and the dose people are exposed to.
Is there a prospect that with more people getting more tattoos, cancers linked to this exposure will occur? Again, we don’t know.
Specific concerns that tattoos might cause or mask skin cancer seem – so far at least – unfounded.
It seems timely to establish a study to follow up on those who have tattoos and how they fare compared with those with a “blank canvas”. The simple truth is, we have no idea what, if any, long-term health effects go with having tattoo ink injected into human skin.
Another complexity is the “DIY tattoo”. Controlling the ink administered by paid tattoo artists in identifiable businesses is one issue. Controlling the ink that comes through online shopping and is administered by enthusiastic amateurs at home is quite another.
So, if you already have tattoos, what should you do? Removing them may not help. The NICNAS report says:
These chemicals can undergo photo degradation under exposure to … solar radiation and lasers.
This means the chemicals, instead of being trapped under the skin, are released into the body. And it’s unclear what effect this might have.
As tattooing becomes increasingly mainstream, we need to ensure those who are considering getting tattooed are fully informed of the risks. And if they wish to proceed, we need to ensure they can do so as safely as possible.
Stopping the use of unsafe ink and related contaminants is a vital first move. This report from NICNAS is an important step towards us getting this house in order.
Terry Slevin is Education and Research Director for Cancer Council Western Australia. He is also Chair of the Cancer Council Australia Occupational and Environmental Cancer Committee. He represents Cancer Council Australia on the Strategic Consultative Committee for The National Industrial Chemical Notification and Assessment Scheme (NICNAS)
by George Dvorsky on Gizmodo, shared by Mario Aguilar to io9
To prevent Zika-infected mosquitoes from taking root in South Carolina, officials in Dorchester County gave the go-ahead to spray a powerful insecticide over the countryside. The effort resulted in the unexpected deaths of millions of bees at a time when these critical pollinators are struggling worldwide.
In France, the final text of a new law on Open Access has been adopted on June 29, 2016. On July 20, the Assemblée Nationale has approved the bill, and it still needs to be voted on by the Sénat on September 27.
A growing share of Americans are reading e-books on tablets and smartphones rather than dedicated e-readers, but print books remain much more popular than books in digital formats
by Menna Elizabeth Jones, Associate professor, University of Tasmania
A healthy devil. Menna Jones
For the past 20 years, an infectious cancer has been killing wild Tasmanian devils, creating a massive challenge for conservationists. But new research, published today in Nature Communications, suggests that devils are evolving rapidly in response to their highly lethal transmissible cancer and that they could ultimately save themselves.
Cancer is usually a disease that arises and dies with its host. In vertebrates, only two known types – Canine Transmissible Venereal Cancer in dogs and Devil Facial Tumour Disease (DFTD) – have taken the extraordinary evolutionary step of becoming transmissible. These cancers can grow not just within their host but can spread to other individuals. Because the cancer cells are all descendants of one mutant cell, the cancer is effectively immortal.
To grow in the new host, the tumour cell must evade detection and rejection by the immune system. Both the devil and dog transmissible cancers have sophisticated mechanisms for hiding from the host’s immune system. Our research suggests that the devil is nevertheless evolving resistance to the disease.
Ecological disaster
The Tasmanian devil is too important to lose – and this would seem careless following the extinction of the thylacine, the world’s largest marsupial predator, in the 1930s. Since the thylacine’s extinction, devils have stepped up to the role of top marsupial predator, keeping numbers of destructive feral cats at bay in Tasmania. With the decline of the devils, invasive species have become more active.
Since it was first detected in northeastern Tasmania in the mid-1990s, DFTD has spread slowly southward and westward. It will reach all parts of Tasmania within a few years; only the far northwest coast and parts of the southwest are still disease-free.
Devil Facial Tumour Disease has spread across the island over two decades.
Menna Jones
DFTD kills most devils at sexual maturity. Before the disease arrived, most devils produced three litters over their lifetime. Most now raise only one.
The cascading effects of the loss of Tasmania’s top predator on the rest of the ecosystem could lead to loss of further species. Already, feral cats have increased activity and small mammals on which cats prey have declined.
Our research has been a truly international effort. We used data collected by Menna Jones at the University of Tasmania since 1999. This archive of tissue samples now represents one of the best resources globally for studying evolution of an emerging infectious disease in wildlife.
Andrew Storfer at Washington State University and Paul Hohenlohe at the University of Idaho compared the frequency of genes in devils in regions before DFTD arrived to devils 8-16 years after DFTD arrived.
We identified significant changes in two small regions in the DNA samples of devils from regions with DFTD. Five of seven genes in the two regions were related to cancer or immune function in other mammals, suggesting that Tasmanian devils are indeed evolving resistance to DFTD. Evolution is often thought of as a slow process, but these changes have occurred in as few as 4–8 generations of devils since disease outbreak.
New infectious diseases put strong pressure on their hosts to evolve, leading to rapid changes in resistance or tolerance. Rapid evolution requires pre-existing genetic variation. Our results are surprising because Tasmanian devils have low levels of genetic diversity.
Evolution doesn’t just act on the devils; it also also acts on the disease. The disease evolves to not kill the host before it can spread to another host, but also to overcome the host’s defences. Over the long term, pathogen (the cause of the disease) and host usually evolve to live together as rabbits and Myxoma virus have evolved together.
Our results suggest that devils in the wild may save themselves through evolution. However, it is essential for managers to develop strategies that help the devils do so. For example, releasing fully susceptible devils that have had no exposure to the disease into populations where resistance is developing is likely to be counterproductive.
DFTD presents a unique opportunity to study the early stages of the evolution of a new disease and transmissible cancer with its animal host. Ultimately, through future research, we may understand how cancers can become transmissible and how their hosts respond.
Menna Elizabeth Jones receives funding from the Australian Research Council, the US National Science Foundation and the Save the Tasmanian Devil Appeal.
Andrew Storfer receives funding from US National Science Foundation
Hamish McCallum receives funding from the US National Science Foundation, the Australian Research Council and the Queensland Government.
Paul Hohenlohe receives funding from the US National Science Foundation and the US National Institutes of Health.
Rodrigo Hamede receives funding from University of Tasmania Foundation, the US National Science Foundation and the Save the Tasmanian devil Program.
School of Biological Sciences, University of Tasmania. Australia
President Obama published an article in the Journal of the American Medical Association today discussing the current state of his health care reform initiatives. Fortunately, the article is not behind a paywall. But JAMA nonetheless asserts their ownership and right to control the article’s use, as they do on all articles they publish, by attaching the following to the article’s PDF.
Unfortunately for JAMA, they have no right to do this. Section 105 of US Copyright law makes clear that works of the US government – and POTUS is a government employee last time I checked – are not eligible for copyright protection in the US (and JAMA is in the US).
17 U.S. Code § 105 – Subject matter of copyright: United States Government works
Copyright protection under this title is not available for any work of the United States Government, but the United States Government is not precluded from receiving and holding copyrights transferred to it by assignment, bequest, or otherwise.
It is completely inexcusable for journals to assert a right they are aware they do not have, thereby undoubtedly leading to people failing to make use of the article in ways that they are clearly legally eligible to do, such as redistributing and reusing the content, as I am doing here.
Special Communication | July 11, 2016
United States Health Care Reform: Progress to Date and Next Steps
Barack Obama, JD1
1President of the United States, Washington, DC
ABSTRACT
Importance The Affordable Care Act is the most important health care legislation enacted in the United States since the creation of Medicare and Medicaid in 1965. The law implemented comprehensive reforms designed to improve the accessibility, affordability, and quality of health care.
Objectives To review the factors influencing the decision to pursue health reform, summarize evidence on the effects of the law to date, recommend actions that could improve the health care system, and identify general lessons for public policy from the Affordable Care Act.
Evidence Analysis of publicly available data, data obtained from government agencies, and published research findings. The period examined extends from 1963 to early 2016.
Findings The Affordable Care Act has made significant progress toward solving long-standing challenges facing the US health care system related to access, affordability, and quality of care. Since the Affordable Care Act became law, the uninsured rate has declined by 43%, from 16.0% in 2010 to 9.1% in 2015, primarily because of the law’s reforms. Research has documented accompanying improvements in access to care (for example, an estimated reduction in the share of nonelderly adults unable to afford care of 5.5 percentage points), financial security (for example, an estimated reduction in debts sent to collection of $600-$1000 per person gaining Medicaid coverage), and health (for example, an estimated reduction in the share of nonelderly adults reporting fair or poor health of 3.4 percentage points). The law has also begun the process of transforming health care payment systems, with an estimated 30% of traditional Medicare payments now flowing through alternative payment models like bundled payments or accountable care organizations. These and related reforms have contributed to a sustained period of slow growth in per-enrollee health care spending and improvements in health care quality. Despite this progress, major opportunities to improve the health care system remain.
Conclusions and Relevance Policy makers should build on progress made by the Affordable Care Act by continuing to implement the Health Insurance Marketplaces and delivery system reform, increasing federal financial assistance for Marketplace enrollees, introducing a public plan option in areas lacking individual market competition, and taking actions to reduce prescription drug costs. Although partisanship and special interest opposition remain, experience with the Affordable Care Act demonstrates that positive change is achievable on some of the nation’s most complex challenges.
INTRODUCTION
Health care costs affect the economy, the federal budget, and virtually every American family’s financial well-being. Health insurance enables children to excel at school, adults to work more productively, and Americans of all ages to live longer, healthier lives. When I took office, health care costs had risen rapidly for decades, and tens of millions of Americans were uninsured. Regardless of the political difficulties, I concluded comprehensive reform was necessary.
The result of that effort, the Affordable Care Act (ACA), has made substantial progress in addressing these challenges. Americans can now count on access to health coverage throughout their lives, and the federal government has an array of tools to bring the rise of health care costs under control. However, the work toward a high-quality, affordable, accessible health care system is not over.
In this Special Communication, I assess the progress the ACA has made toward improving the US health care system and discuss how policy makers can build on that progress in the years ahead. I close with reflections on what my administration’s experience with the ACA can teach about the potential for positive change in health policy in particular and public policy generally.
IMPETUS FOR HEALTH REFORM
In my first days in office, I confronted an array of immediate challenges associated with the Great Recession. I also had to deal with one of the nation’s most intractable and long-standing problems, a health care system that fell far short of its potential. In 2008, the United States devoted 16% of the economy to health care, an increase of almost one-quarter since 1998 (when 13% of the economy was spent on health care), yet much of that spending did not translate into better outcomes for patients.1– 4 The health care system also fell short on quality of care, too often failing to keep patients safe, waiting to treat patients when they were sick rather than focusing on keeping them healthy, and delivering fragmented, poorly coordinated care.5,6
Moreover, the US system left more than 1 in 7 Americans without health insurance coverage in 2008.7 Despite successful efforts in the 1980s and 1990s to expand coverage for specific populations, like children, the United States had not seen a large, sustained reduction in the uninsured rate since Medicare and Medicaid began (Figure 18– 10). The United States’ high uninsured rate had negative consequences for uninsured Americans, who experienced greater financial insecurity, barriers to care, and odds of poor health and preventable death; for the health care system, which was burdened with billions of dollars in uncompensated care; and for the US economy, which suffered, for example, because workers were concerned about joining the ranks of the uninsured if they sought additional education or started a business.11– 16 Beyond these statistics were the countless, heartbreaking stories of Americans who struggled to access care because of a broken health insurance system. These included people like Natoma Canfield, who had overcome cancer once but had to discontinue her coverage due to rapidly escalating premiums and found herself facing a new cancer diagnosis uninsured.17
Figure 1.
Percentage of Individuals in the United States Without Health Insurance, 1963-2015
Data are derived from the National Health Interview Survey and, for years prior to 1982, supplementary information from other survey sources and administrative records. The methods used to construct a comparable series spanning the entire period build on those in Cohen et al8 and Cohen9 and are described in detail in Council of Economic Advisers 2014.10 For years 1989 and later, data are annual. For prior years, data are generally but not always biannual. ACA indicates Affordable Care Act.
In 2009, during my first month in office, I extended the Children’s Health Insurance Program and soon thereafter signed the American Recovery and Reinvestment Act, which included temporary support to sustain Medicaid coverage as well as investments in health information technology, prevention, and health research to improve the system in the long run. In the summer of 2009, I signed the Tobacco Control Act, which has contributed to a rapid decline in the rate of smoking among teens, from 19.5% in 2009 to 10.8% in 2015, with substantial declines among adults as well.7,18
Beyond these initial actions, I decided to prioritize comprehensive health reform not only because of the gravity of these challenges but also because of the possibility for progress. Massachusetts had recently implemented bipartisan legislation to expand health insurance coverage to all its residents. Leaders in Congress had recognized that expanding coverage, reducing the level and growth of health care costs, and improving quality was an urgent national priority. At the same time, a broad array of health care organizations and professionals, business leaders, consumer groups, and others agreed that the time had come to press ahead with reform.19 Those elements contributed to my decision, along with my deeply held belief that health care is not a privilege for a few, but a right for all. After a long debate with well-documented twists and turns, I signed the ACA on March 23, 2010.
PROGRESS UNDER THE ACA
The years following the ACA’s passage included intense implementation efforts, changes in direction because of actions in Congress and the courts, and new opportunities such as the bipartisan passage of the Medicare Access and CHIP Reauthorization Act (MACRA) in 2015. Rather than detail every development in the intervening years, I provide an overall assessment of how the health care system has changed between the ACA’s passage and today.
The evidence underlying this assessment was obtained from several sources. To assess trends in insurance coverage, this analysis relies on publicly available government and private survey data, as well as previously published analyses of survey and administrative data. To assess trends in health care costs and quality, this analysis relies on publicly available government estimates and projections of health care spending; publicly available government and private survey data; data on hospital readmission rates provided by the Centers for Medicare & Medicaid Services; and previously published analyses of survey, administrative, and clinical data. The dates of the data used in this assessment range from 1963 to early 2016.
The ACA has succeeded in sharply increasing insurance coverage. Since the ACA became law, the uninsured rate has declined by 43%, from 16.0% in 2010 to 9.1% in 2015,7 with most of that decline occurring after the law’s main coverage provisions took effect in 2014 (Figure 18– 10). The number of uninsured individuals in the United States has declined from 49 million in 2010 to 29 million in 2015. This is by far the largest decline in the uninsured rate since the creation of Medicare and Medicaid 5 decades ago. Recent analyses have concluded these gains are primarily because of the ACA, rather than other factors such as the ongoing economic recovery.20,21 Adjusting for economic and demographic changes and other underlying trends, the Department of Health and Human Services estimated that 20 million more people had health insurance in early 2016 because of the law.22
Each of the law’s major coverage provisions—comprehensive reforms in the health insurance market combined with financial assistance for low- and moderate-income individuals to purchase coverage, generous federal support for states that expand their Medicaid programs to cover more low-income adults, and improvements in existing insurance coverage—has contributed to these gains. States that decided to expand their Medicaid programs saw larger reductions in their uninsured rates from 2013 to 2015, especially when those states had large uninsured populations to start with (Figure 223). However, even states that have not adopted Medicaid expansion have seen substantial reductions in their uninsured rates, indicating that the ACA’s other reforms are increasing insurance coverage. The law’s provision allowing young adults to stay on a parent’s plan until age 26 years has also played a contributing role, covering an estimated 2.3 million people after it took effect in late 2010.22
Figure 2.
Decline in Adult Uninsured Rate From 2013 to 2015 vs 2013 Uninsured Rate by State
Data are derived from the Gallup-Healthways Well-Being Index as reported by Witters23 and reflect uninsured rates for individuals 18 years or older. Dashed lines reflect the result of an ordinary least squares regression relating the change in the uninsured rate from 2013 to 2015 to the level of the uninsured rate in 2013, run separately for each group of states. The 29 states in which expanded coverage took effect before the end of 2015 were categorized as Medicaid expansion states, and the remaining 21 states were categorized as Medicaid nonexpansion states.
Early evidence indicates that expanded coverage is improving access to treatment, financial security, and health for the newly insured. Following the expansion through early 2015, nonelderly adults experienced substantial improvements in the share of individuals who have a personal physician (increase of 3.5 percentage points) and easy access to medicine (increase of 2.4 percentage points) and substantial decreases in the share who are unable to afford care (decrease of 5.5 percentage points) and reporting fair or poor health (decrease of 3.4 percentage points) relative to the pre-ACA trend.24 Similarly, research has found that Medicaid expansion improves the financial security of the newly insured (for example, by reducing the amount of debt sent to a collection agency by an estimated $600-$1000 per person gaining Medicaid coverage).26,27 Greater insurance coverage appears to have been achieved without negative effects on the labor market, despite widespread predictions that the law would be a “job killer.” Private-sector employment has increased in every month since the ACA became law, and rigorous comparisons of Medicaid expansion and nonexpansion states show no negative effects on employment in expansion states.28– 30
The law has also greatly improved health insurance coverage for people who already had it. Coverage offered on the individual market or to small businesses must now include a core set of health care services, including maternity care and treatment for mental health and substance use disorders, services that were sometimes not covered at all previously.31 Most private insurance plans must now cover recommended preventive services without cost-sharing, an important step in light of evidence demonstrating that many preventive services were underused.5,6 This includes women’s preventive services, which has guaranteed an estimated 55.6 million women coverage of services such as contraceptive coverage and screening and counseling for domestic and interpersonal violence.32 In addition, families now have far better protection against catastrophic costs related to health care. Lifetime limits on coverage are now illegal and annual limits typically are as well. Instead, most plans must cap enrollees’ annual out-of-pocket spending, a provision that has helped substantially reduce the share of people with employer-provided coverage lacking real protection against catastrophic costs (Figure 333). The law is also phasing out the Medicare Part D coverage gap. Since 2010, more than 10 million Medicare beneficiaries have saved more than $20 billion as a result.34
Figure 3.
Percentage of Workers With Employer-Based Single Coverage Without an Annual Limit on Out-of-pocket Spending
Data from the Kaiser Family Foundation/Health Research and Education Trust Employer Health Benefits Survey.33
Before the ACA, the health care system was dominated by “fee-for-service” payment systems, which often penalized health care organizations and health care professionals who find ways to deliver care more efficiently, while failing to reward those who improve the quality of care. The ACA has changed the health care payment system in several important ways. The law modified rates paid to many that provide Medicare services and Medicare Advantage plans to better align them with the actual costs of providing care. Research on how past changes in Medicare payment rates have affected private payment rates implies that these changes in Medicare payment policy are helping decrease prices in the private sector as well.35,36 The ACA also included numerous policies to detect and prevent health care fraud, including increased scrutiny prior to enrollment in Medicare and Medicaid for health care entities that pose a high risk of fraud, stronger penalties for crimes involving losses in excess of $1 million, and additional funding for antifraud efforts. The ACA has also widely deployed “value-based payment” systems in Medicare that tie fee-for-service payments to the quality and efficiency of the care delivered by health care organizations and health care professionals. In parallel with these efforts, my administration has worked to foster a more competitive market by increasing transparency around the prices charged and the quality of care delivered.
Most importantly over the long run, the ACA is moving the health care system toward “alternative payment models” that hold health care entities accountable for outcomes. These models include bundled payment models that make a single payment for all of the services provided during a clinical episode and population-based models like accountable care organizations (ACOs) that base payment on the results health care organizations and health care professionals achieve for all of their patients’ care. The law created the Center for Medicare and Medicaid Innovation (CMMI) to test alternative payment models and bring them to scale if they are successful, as well as a permanent ACO program in Medicare. Today, an estimated 30% of traditional Medicare payments flow through alternative payment models that broaden the focus of payment beyond individual services or a particular entity, up from essentially none in 2010.37 These models are also spreading rapidly in the private sector, and their spread will likely be accelerated by the physician payment reforms in MACRA.38,39
Trends in health care costs and quality under the ACA have been promising (Figure 41,40). From 2010 through 2014, mean annual growth in real per-enrollee Medicare spending has actually been negative, down from a mean of 4.7% per year from 2000 through 2005 and 2.4% per year from 2006 to 2010 (growth from 2005 to 2006 is omitted to avoid including the rapid growth associated with the creation of Medicare Part D).1,40 Similarly, mean real per-enrollee growth in private insurance spending has been 1.1% per year since 2010, compared with a mean of 6.5% from 2000 through 2005 and 3.4% from 2005 to 2010.1,40
Figure 4.
Rate of Change in Real per-Enrollee Spending by Payer
Data are derived from the National Health Expenditure Accounts.1 Inflation adjustments use the Gross Domestic Product Price Index reported in the National Income and Product Accounts.40 The mean growth rate for Medicare spending reported for 2005 through 2010 omits growth from 2005 to 2006 to exclude the effect of the creation of Medicare Part D.
As a result, health care spending is likely to be far lower than expected. For example, relative to the projections the Congressional Budget Office (CBO) issued just before I took office, CBO now projects Medicare to spend 20%, or about $160 billion, less in 2019 alone.41,42 The implications for families’ budgets of slower growth in premiums have been equally striking. Had premiums increased since 2010 at the same mean rate as the preceding decade, the mean family premium for employer-based coverage would have been almost $2600 higher in 2015.33 Employees receive much of those savings through lower premium costs, and economists generally agree that those employees will receive the remainder as higher wages in the long run.43 Furthermore, while deductibles have increased in recent years, they have increased no faster than in the years preceding 2010.44 Multiple sources also indicate that the overall share of health care costs that enrollees in employer coverage pay out of pocket has been close to flat since 2010 (Figure 545– 48), most likely because the continued increase in deductibles has been canceled out by a decline in co-payments.
Figure 5.
Out-of-pocket Spending as a Percentage of Total Health Care Spending for Individuals Enrolled in Employer-Based Coverage
Data for the series labeled Medical Expenditure Panel Survey (MEPS) were derived from MEPS Household Component and reflect the ratio of out-of-pocket expenditures to total expenditures for nonelderly individuals reporting full-year employer coverage. Data for the series labeled Health Care Cost Institute (HCCI) were derived from the analysis of the HCCI claims database reported in Herrera et al,45 HCCI 2015,46 and HCCI 201547; to capture data revisions, the most recent value reported for each year was used. Data for the series labeled Claxton et al were derived from the analyses of the Trueven Marketscan claims database reported by Claxton et al 2016.48
At the same time, the United States has seen important improvements in the quality of care. The rate of hospital-acquired conditions (such as adverse drug events, infections, and pressure ulcers) has declined by 17%, from 145 per 1000 discharges in 2010 to 121 per 1000 discharges in 2014.49 Using prior research on the relationship between hospital-acquired conditions and mortality, the Agency for Healthcare Research and Quality has estimated that this decline in the rate of hospital-acquired conditions has prevented a cumulative 87 000 deaths over 4 years.49 The rate at which Medicare patients are readmitted to the hospital within 30 days after discharge has also decreased sharply, from a mean of 19.1% during 2010 to a mean of 17.8% during 2015 (Figure 6; written communication; March 2016; Office of Enterprise Data and Analytics, Centers for Medicare & Medicaid Services). The Department of Health and Human Services has estimated that lower hospital readmission rates resulted in 565 000 fewer total readmissions from April 2010 through May 2015.50,51
Data were provided by the Centers for Medicare & Medicaid Services (written communication; March 2016). The plotted series reflects a 12-month moving average of the hospital readmission rates reported for discharges occurring in each month.
While the Great Recession and other factors played a role in recent trends, the Council of Economic Advisers has found evidence that the reforms introduced by the ACA helped both slow health care cost growth and drive improvements in the quality of care.44,52 The contribution of the ACA’s reforms is likely to increase in the years ahead as its tools are used more fully and as the models already deployed under the ACA continue to mature.
BUILDING ON PROGRESS TO DATE
I am proud of the policy changes in the ACA and the progress that has been made toward a more affordable, high-quality, and accessible health care system. Despite this progress, too many Americans still strain to pay for their physician visits and prescriptions, cover their deductibles, or pay their monthly insurance bills; struggle to navigate a complex, sometimes bewildering system; and remain uninsured. More work to reform the health care system is necessary, with some suggestions offered below.
First, many of the reforms introduced in recent years are still some years from reaching their maximum effect. With respect to the law’s coverage provisions, these early years’ experience demonstrate that the Health Insurance Marketplace is a viable source of coverage for millions of Americans and will be for decades to come. However, both insurers and policy makers are still learning about the dynamics of an insurance market that includes all people regardless of any preexisting conditions, and further adjustments and recalibrations will likely be needed, as can be seen in some insurers’ proposed Marketplace premiums for 2017. In addition, a critical piece of unfinished business is in Medicaid. As of July 1, 2016, 19 states have yet to expand their Medicaid programs. I hope that all 50 states take this option and expand coverage for their citizens in the coming years, as they did in the years following the creation of Medicaid and CHIP.
With respect to delivery system reform, the reorientation of the US health care payment systems toward quality and accountability has made significant strides forward, but it will take continued hard work to achieve my administration’s goal of having at least half of traditional Medicare payments flowing through alternative payment models by the end of 2018. Tools created by the ACA—including CMMI and the law’s ACO program—and the new tools provided by MACRA will play central roles in this important work. In parallel, I expect continued bipartisan support for identifying the root causes and cures for diseases through the Precision Medicine and BRAIN initiatives and the Cancer Moonshot, which are likely to have profound benefits for the 21st-century US health care system and health outcomes.
Second, while the ACA has greatly improved the affordability of health insurance coverage, surveys indicate that many of the remaining uninsured individuals want coverage but still report being unable to afford it.53,54 Some of these individuals may be unaware of the financial assistance available under current law, whereas others would benefit from congressional action to increase financial assistance to purchase coverage, which would also help middle-class families who have coverage but still struggle with premiums. The steady-state cost of the ACA’s coverage provisions is currently projected to be 28% below CBO’s original projections, due in significant part to lower-than-expected Marketplace premiums, so increased financial assistance could make coverage even more affordable while still keeping federal costs below initial estimates.55,56
Third, more can and should be done to enhance competition in the Marketplaces. For most Americans in most places, the Marketplaces are working. The ACA supports competition and has encouraged the entry of hospital-based plans, Medicaid managed care plans, and other plans into new areas. As a result, the majority of the country has benefited from competition in the Marketplaces, with 88% of enrollees living in counties with at least 3 issuers in 2016, which helps keep costs in these areas low.57,58 However, the remaining 12% of enrollees live in areas with only 1 or 2 issuers. Some parts of the country have struggled with limited insurance market competition for many years, which is one reason that, in the original debate over health reform, Congress considered and I supported including a Medicare-like public plan. Public programs like Medicare often deliver care more cost-effectively by curtailing administrative overhead and securing better prices from providers.59,60 The public plan did not make it into the final legislation. Now, based on experience with the ACA, I think Congress should revisit a public plan to compete alongside private insurers in areas of the country where competition is limited. Adding a public plan in such areas would strengthen the Marketplace approach, giving consumers more affordable options while also creating savings for the federal government.61
Fourth, although the ACA included policies to help address prescription drug costs, like more substantial Medicaid rebates and the creation of a pathway for approval of biosimilar drugs, those costs remain a concern for Americans, employers, and taxpayers alike—particularly in light of the 12% increase in prescription drug spending that occurred in 2014.1 In addition to administrative actions like testing new ways to pay for drugs, legislative action is needed.62 Congress should act on proposals like those included in my fiscal year 2017 budget to increase transparency around manufacturers’ actual production and development costs, to increase the rebates manufacturers are required to pay for drugs prescribed to certain Medicare and Medicaid beneficiaries, and to give the federal government the authority to negotiate prices for certain high-priced drugs.63
There is another important role for Congress: it should avoid moving backward on health reform. While I have always been interested in improving the law—and signed 19 bills that do just that—my administration has spent considerable time in the last several years opposing more than 60 attempts to repeal parts or all of the ACA, time that could have been better spent working to improve our health care system and economy. In some instances, the repeal efforts have been bipartisan, including the effort to roll back the excise tax on high-cost employer-provided plans. Although this provision can be improved, such as through the reforms I proposed in my budget, the tax creates strong incentives for the least-efficient private-sector health plans to engage in delivery system reform efforts, with major benefits for the economy and the budget. It should be preserved.64 In addition, Congress should not advance legislation that undermines the Independent Payment Advisory Board, which will provide a valuable backstop if rapid cost growth returns to Medicare.
LESSONS FOR FUTURE POLICY MAKERS
While historians will draw their own conclusions about the broader implications of the ACA, I have my own. These lessons learned are not just for posterity: I have put them into practice in both health care policy and other areas of public policy throughout my presidency.
The first lesson is that any change is difficult, but it is especially difficult in the face of hyperpartisanship. Republicans reversed course and rejected their own ideas once they appeared in the text of a bill that I supported. For example, they supported a fully funded risk-corridor program and a public plan fallback in the Medicare drug benefit in 2003 but opposed them in the ACA. They supported the individual mandate in Massachusetts in 2006 but opposed it in the ACA. They supported the employer mandate in California in 2007 but opposed it in the ACA—and then opposed the administration’s decision to delay it. Moreover, through inadequate funding, opposition to routine technical corrections, excessive oversight, and relentless litigation, Republicans undermined ACA implementation efforts. We could have covered more ground more quickly with cooperation rather than obstruction. It is not obvious that this strategy has paid political dividends for Republicans, but it has clearly come at a cost for the country, most notably for the estimated 4 million Americans left uninsured because they live in GOP-led states that have yet to expand Medicaid.65
The second lesson is that special interests pose a continued obstacle to change. We worked successfully with some health care organizations and groups, such as major hospital associations, to redirect excessive Medicare payments to federal subsidies for the uninsured. Yet others, like the pharmaceutical industry, oppose any change to drug pricing, no matter how justifiable and modest, because they believe it threatens their profits.66 We need to continue to tackle special interest dollars in politics. But we also need to reinforce the sense of mission in health care that brought us an affordable polio vaccine and widely available penicillin.
The third lesson is the importance of pragmatism in both legislation and implementation. Simpler approaches to addressing our health care problems exist at both ends of the political spectrum: the single-payer model vs government vouchers for all. Yet the nation typically reaches its greatest heights when we find common ground between the public and private good and adjust along the way. That was my approach with the ACA. We engaged with Congress to identify the combination of proven health reform ideas that could pass and have continued to adapt them since. This includes abandoning parts that do not work, like the voluntary long-term care program included in the law. It also means shutting down and restarting a process when it fails. When HealthCare.gov did not work on day 1, we brought in reinforcements, were brutally honest in assessing problems, and worked relentlessly to get it operating. Both the process and the website were successful, and we created a playbook we are applying to technology projects across the government.
While the lessons enumerated above may seem daunting, the ACA experience nevertheless makes me optimistic about this country’s capacity to make meaningful progress on even the biggest public policy challenges. Many moments serve as reminders that a broken status quo is not the nation’s destiny. I often think of a letter I received from Brent Brown of Wisconsin. He did not vote for me and he opposed “ObamaCare,” but Brent changed his mind when he became ill, needed care, and got it thanks to the law.67 Or take Governor John Kasich’s explanation for expanding Medicaid: “For those that live in the shadows of life, those who are the least among us, I will not accept the fact that the most vulnerable in our state should be ignored. We can help them.”68 Or look at the actions of countless health care providers who have made our health system more coordinated, quality-oriented, and patient-centered. I will repeat what I said 4 years ago when the Supreme Court upheld the ACA: I am as confident as ever that looking back 20 years from now, the nation will be better off because of having the courage to pass this law and persevere. As this progress with health care reform in the United States demonstrates, faith in responsibility, belief in opportunity, and ability to unite around common values are what makes this nation great.
ARTICLE INFORMATION
Corresponding Author: Barack Obama, JD, The White House, 1600 Pennsylvania Ave NW, Washington, DC 20500 (press@who.eop.gov).
Additional Contributions: I thank Matthew Fiedler, PhD, and Jeanne Lambrew, PhD, who assisted with planning, writing, and data analysis. I also thank Kristie Canegallo, MA; Katie Hill, BA; Cody Keenan, MPP; Jesse Lee, BA; and Shailagh Murray, MS, who assisted with editing the manuscript. All of the individuals who assisted with the preparation of the manuscript are employed by the Executive Office of the President.
Anderson GF, Frogner BK. Health spending in OECD countries: obtaining value per dollar. Health Aff (Millwood). 2008;27(6):1718-1727. PubMed | Link to Article
3
Fisher ES, Wennberg DE, Stukel TA, Gottlieb DJ, Lucas FL, Pinder EL. The implications of regional variations in Medicare spending: part 1: the content, quality, and accessibility of care. Ann Intern Med. 2003;138(4):273-287. PubMed | Link to Article
4
Fisher ES, Wennberg DE, Stukel TA, Gottlieb DJ, Lucas FL, Pinder EL. The implications of regional variations in Medicare spending: part 2: health outcomes and satisfaction with care. Ann Intern Med. 2003;138(4):288-298. PubMed | Link to Article
5
McGlynn EA, Asch SM, Adams J, et al. The quality of health care delivered to adults in the United States. N Engl J Med. 2003;348(26):2635-2645. PubMed | Link to Article
Cohen RA, Martinez ME, Zammitti EP. Early release of selected estimates based on data from the National Health Interview Survey, 2015. National Center for Health Statistics.http://www.cdc.gov/nchs/nhis/releases/released201605.htm. Published May 24, 2016. Accessed June 14, 2016.
8
Cohen RA, Makuc DM, Bernstein AB, Bilheimer LT, Powell-Griner E. Health insurance coverage trends, 1959-2007: estimates from the National Health Interview Survey. National Center for Health Statistics.http://www.cdc.gov/nchs/data/nhsr/nhsr017.pdf. Published July 1, 2009. Accessed June 14, 2016.
Baicker K, Taubman SL, Allen HL, et al; Oregon Health Study Group. The Oregon experiment: effects of Medicaid on clinical outcomes. N Engl J Med. 2013;368(18):1713-1722. PubMed | Link to Article
12
Sommers BD, Baicker K, Epstein AM. Mortality and access to care among adults after state Medicaid expansions. N Engl J Med. 2012;367(11):1025-1034. PubMed | Link to Article
13
Sommers BD, Long SK, Baicker K. Changes in mortality after Massachusetts health care reform: a quasi-experimental study. Ann Intern Med. 2014;160(9):585-593. PubMed | Link to Article
14
Hadley J, Holahan J, Coughlin T, Miller D. Covering the uninsured in 2008: current costs, sources of payment, and incremental costs. Health Aff (Millwood). 2008;27(5):w399-w415. PubMed | Link to Article
15
Fairlie RW, Kapur K, Gates S. Is employer-based health insurance a barrier to entrepreneurship? J Health Econ. 2011;30(1):146-162. PubMed | Link to Article
16
Dillender M. Do more health insurance options lead to higher wages? evidence from states extending dependent coverage. J Health Econ. 2014;36:84-97. PubMed | Link to Article
Oberlander J. Long time coming: why health reform finally passed. Health Aff (Millwood). 2010;29(6):1112-1116. PubMed | Link to Article
20
Courtemanche C, Marton J, Ukert B, Yelowtize A, Zapata D. Impacts of the Affordable Care Act on health insurance coverage in Medicaid expansion and non-expansion states [NBER working paper No. 22182]. National Bureau of Economic Research. http://www.nber.org/papers/w22182. Published April 2016. Accessed June 14, 2016.
21
Blumberg LJ, Garrett B, Holahan J. Estimating the counterfactual: how many uninsured adults would there be today without the ACA? Inquiry. 2016;53(3):1-13. PubMed
22
Uberoi N, Finegold K, Gee E. Health insurance coverage and the Affordable Care Act, 2010-2016. Office of the Assistant Secretary for Planning and Evaluation, US Department of Health and Human Services.https://aspe.hhs.gov/sites/default/files/pdf/187551/ACA2010-2016.pdf. Published March 3, 2016. Accessed June 14, 2016.
Sommers BD, Gunja MZ, Finegold K, Musco T. Changes in self-reported insurance coverage, access to care, and health under the Affordable Care Act. JAMA. 2015;314(4):366-374. PubMed | Link to Article
25
Shartzer A, Long SK, Anderson N. Access to care and affordability have improved following Affordable Care Act implementation; problems remain. Health Aff (Millwood). 2016;35(1):161-168. PubMed | Link to Article
Hu L, Kaestner R, Mazumder B, Miller S, Wong A. The effect of the Patient Protection and Affordable Care Act Medicaid expansions on financial well-being [NBER working paper No. 22170]. National Bureau of Economic Research. http://www.nber.org/papers/w22170. Published April 2016. Accessed June 14, 2016.
28
Bureau of Labor Statistics. Employment, hours, and earnings from the Current Employment Statistics survey (national): Series ID CES0500000001. http://data.bls.gov/timeseries/CES0500000001. Accessed June 14, 2016.
29
Kaestner R, Garrett B, Gangopadhyaya A, Fleming C. Effects of the ACA Medicaid expansions on health insurance coverage and labor supply [NBER working paper No. 21836]. National Bureau of Economic Research.http://www.nber.org/papers/w21836. Published December 2015. Accessed June 14, 2016.
Simmons A, Taylor J, Finegold K, Yabroff R, Gee E, Chappel E. The Affordable Care Act: promoting better health for women. Office of the Assistant Secretary for Planning and Evaluation, US Department of Health and Human Services. https://aspe.hhs.gov/pdf-report/affordable-care-act-promoting-better-health-women. Published June 14, 2016. Accessed June 18, 2016.
White C. Contrary to cost-shift theory, lower Medicare hospital payment rates for inpatient care lead to lower private payment rates. Health Aff (Millwood). 2013;32(5):935-943. PubMed | Link to Article
Board of Trustees of the Federal Hospital Insurance and Federal Supplementary Medical Insurance Trust Funds.2015 Annual Report of the Board of Trustees of the Federal Hospital Insurance and Federal Supplementary Medical Insurance Trust Funds. Washington, DC: Centers for Medicare & Medicaid Services; 2015.
Congressional Budget Office. The budget and economic outlook: fiscal years 2009 to 2019.https://www.cbo.gov/publication/41753. Published January 7, 2009. Accessed June 14, 2016.
42
Congressional Budget Office. Updated budget projections: 2016 to 2026. https://www.cbo.gov/publication/51384. Published March 24, 2016. Accessed June 14, 2016.
43
Congressional Budget Office. Private Health Insurance Premiums and Federal Policy. Washington, DC: Congressional Budget Office; 2016.
Herrera CN, Gaynor M, Newman D, Town RJ, Parente ST. Trends underlying employer-sponsored health insurance growth for Americans younger than age sixty-five. Health Aff (Millwood). 2013;32(10):1715-1722. PubMed | Link to Article
Congressional Budget Office. HR 4872, Reconciliation Act of 2010 (Final Health Care Legislation).https://www.cbo.gov/publication/21351. Published March 20, 2010. Accessed June 14, 2016.
56
Congressional Budget Office. Federal subsidies for health insurance coverage for people under age 65: 2016 to 2026. https://www.cbo.gov/publication/51385. Published March 24, 2016. Accessed June 14, 2016.
Avery K, Gardner M, Gee E, Marchetti-Bowick E, McDowell A, Sen A. Health plan choice and premiums in the 2016 Health Insurance Marketplace. Office of the Assistant Secretary for Planning and Evaluation, US Department of Health and Human Services. https://aspe.hhs.gov/pdf-report/health-plan-choice-and-premiums-2016-health-insurance-marketplace. Published October 30, 2015. Accessed June 14, 2016.
59
Congressional Budget Office. Key issues in analyzing major health insurance proposals.https://www.cbo.gov/publication/41746. Published December 18, 2008. Accessed June 14, 2016.
60
Wallace J, Song Z. Traditional Medicare versus private insurance: how spending, volume, and price change at age sixty-five. Health Aff (Millwood). 2016;35(5):864-872. PubMed | Link to Article
As a professor of Russian literature, I’ve come to realize that it’s never a good sign when real life resembles a Fyodor Dostoevsky novel.
Donald Trump’s presidential campaign, with its riotous rhetoric and steady stream of scandals, calls to mind Dostoevsky’s most political novel, “Demons,” written in 1872. In it, the writer wanted to warn readers about the destructive force of demagoguery and unchecked rhetoric, and his cautionary messages – largely influenced by 19th-century Russian political chaos – resonate in our present political climate.
To show his readers just how bad things could get if they didn’t pay attention, Dostoevsky linked his political nightmare to unhinged impulses and the breakdown of civility.
A passion for destruction
Dostoevsky was as addicted to newspapers as some of us are to social media, and he often plucked crises and violence right from the headlines, refashioning them for his fiction.
Russia during the 1860s and 1870s – the heyday of the author’s career – was experiencing massive socioeconomic instability. Tsar Alexander II’s Emancipation of the Serfs freed Russian peasants from a form of class bondage, while the subsequent Great Reforms aimed to restructure the executive and judidical branches, as well as the military, tax code and education system. The reforms were supposed to modernize the country by dragging it out of the caste-like system of estates and legal privilege. But it didn’t do much to improve the economic lot of the peasant.
It was a reversal of America’s present political landscape. While today there’s simmering discontent from the right, in 19th-century Russia it was leftists who were enraged. They were angered by the reforms for not going far enough and had lost hope in the government’s ability to produce meaningful change.
Sergei Nechaev influenced Dostoevsky’s Pyotr Verkhovensky.
Wikimedia Commons
One of the only unifying ideas among the more radical left-wing political factions of the period was the belief that the tsarist regime must be eliminated. Important public figures, like Russian anarchist Mikhail Bakunin, advocated for destruction of the status quo as an end greater than all ideologies. As Bakunin famously exhorted: “The passion for destruction is a creative passion, too.”
Bakunin’s conviction that a new world could rise only from the ashes of tsarism was actually put into practice by his one-time disciple, Sergei Nechaev, who was the inspiration for Dostoevsky’s protagonist in “Demons,” Pyotr Verkhovensky.
A slippery slope from incivility to violence
In 1869, Nechaev orchestrated the murder of a young student, an event that so shocked and angered Dostoevsky that it became the basis for “Demons.”
The novel begins in a boring provincial backwater inhabited by middle-aged people and ineffectual young liberals, all engrossed in their romantic lives. Pyotr Verkhovensky arrives and persuades many of these same characters to join his underground revolutionary society. Passions are stirred and the local order destabilized as the town enters a downward spiral that concludes with arson and several murders.
What’s most relevant to our time in “Demons” is not its ideologues but the anti-intellectual and impulse-driven nature of Pyotr’s rebellion. In Pyotr, Dostoevsky created a demagogue and pure nihilist, a political figure who appeals to people’s baser desires. Under his influence, the townspeople lose all impulse control and grow reckless, rebelling against all conventions of decency for a good laugh. At one point they desecrate a sacred icon; at another, they gleefully gather around the body of someone who has committed suicide and eat the food he’s left behind.
If their pranks, insults and disorder seem harmless, the decline in the level of public discourse act as a precursor to the violent and destructive acts at the novel’s conclusion. A skilled psychological writer, Dostoevsky never saw violence as divorced from normal human behavior. What’s most haunting about his works is just how close otherwise ordinary people are from doing extraordinarily awful things.
In “Demons,” narrative tensions escalate in a deliberately gradual way. What begins as minor impoliteness becomes scandal, arson, murder and suicide. Dostoevsky is essentially saying that criminal acts are rooted in social transgression; uncivil behavior facilitates scapegoating, dehumanization and, eventually, violence.
‘Make America Great Again!’
Donald Trump’s unconventional campaign for president powerfully evokes Dostoevsky’s novel. Aside from his pro-gun and anti-immigration positions, Trump doesn’t offer many concrete political plans. As we evaluate what motivated 14 million Americans to vote for him in the primaries, we might consider new research showing that his candidacy has a primarily emotion-based – rather than ideological or economical – appeal. There are notable anti-establishment sentiments among his supporters; many are disaffected, middle-aged white people who believe that American institutions aren’t working on their behalf.
And while his notorious campaign motto “Make America Great Again” is framed in a positive way, it actually advances a version of Bakunin’s creative destruction. It stands for purging the establishment, for recreating a nostalgia-tinged version of some lost, past America. We’ve already seen this destructive drive in its more Nechaevist, low-brow form at Trump rallies, where several people have been attacked.
There’s another aspect of Trump’s popularity that ties him to Dostoevsky’s “Demons.” Trump, in the way he carries himself, embodies the complete disavowal of impulse control we see in the novel. Unlike most political candidates, he speaks off the cuff, simultaneously reflecting and stoking the anger and pessimism of his supporters.
For instance, he said he wanted to “hit” some of the speakers who criticized him at the Democratic National Convention; in his words, there’s anger, a need to provoke and deep-seated irreverence. His supporters feel empowered by this. Without weighing his policies, they’re viscerally drawn to the spectacle of his candidacy, like the townspeople following Pyotr Verkhovensky in “Demons” who delight in the gossip and scandals he creates.
To complete the parallel, we might turn to the novel’s ending, which could have a sobering effect. Basic incivility gives way to an anarchic vision of creative destruction; many die or lose their minds due to Pyotr’s machinations. At one point, seemingly without thinking, crowds crush a female character to death because they falsely believe she’s responsible for the violence in town.
When audiences at Trump rallies verbalize violence by screaming “Lock her up” and “Kill her,” or when Donald Trump – either wittingly or unwittingly – advocates Second Amendment violence, I wonder whether they aren’t coming dangerously close to the primal violence of “Demons.”
Ani Kokobobo does not work for, consult, own shares in or receive funding from any company or organization that would benefit from this article, and has disclosed no relevant affiliations beyond the academic appointment above.
by Maddie Stone on Gizmodo, shared by Katie Drummond to io9
It’s a scorching midsummer day, and the sawgrass is still under a pale blue sky. Waist-deep in water and sinking slowly into the muck, I fend off mosquitos as a man from South Florida’s Water Management District mixes a bag of salt into a hot tub-sized bucket on the side of the road. Thirty feet away in the marsh, another city official wearing waders and a bug hat stands on a narrow steel walkway, dangling the end of a long hose over a plexiglass chamber.
Stand down, Rob Zombie—your reign of terror over all horror movies set within deranged carnival environments is getting some competition. Jennifer Chambers Lynch, whose genre chops include episodes of The Walking Dead and Teen Wolf, has been tapped to helm a Halloween-themed thriller called Hellfest.
The Death of Cock Robin, also known as The Death and Burial of Cock Robin is a somewhat macabre English nursery rhyme describing the murder and the funeral of a robin.
Help is on the way, both in person and online. At ALA Annual 2016, the Copyright Answer booth is back. On Saturday and Sunday only, from 10am – 4pm, conveniently located in the Orange County Convention Center outside of the Exhibit Hall and staffed by copyright librarian experts, stop by and pour your heart out. What copyright issue is troubling you? Feel like venting? We have been there and done that. We will listen, and provide non-legal, but well informed advice.
If you can’t make it to Orlando, don’t pout. The Copyright Advisory Network (CAN) is back. Any time, day or night, post your copyright question or issue on the CAN forum. Within 24 hours (except holidays and weekends), one of our knowledgeable copyright scholars will respond to your query. We also have online copyright tools for figuring out when materials are in the public domain, conducting a fair use analysis and more. By the way, it’s all FREE. You will never be asked to pay a fee or take a drug test.
These services are brought to you by fellow librarians who are members of the Office for Information Technology Policy (OITP) Copyright Education Subcommittee. Our primary mission is to help librarians who find themselves on the copyright front lines navigate the mine field.
One of Disney’s most underrated films, The Rocketeer, is finally getting the respect it deserves. The Hollywood Reporter says the company is prepping a brand new sequel/reboot called The Rocketeers and the new hero is an African-American woman.
Get your dance moves in order—you know the ones—because here’s our best look yet at Fox’s new production of the Rocky Horror Picture Show It’s got more Frank-N-Furter, more Time Warp, and yes, even a teeny tiny bit of Tim Curry.
by Maddie Stone on Gizmodo, shared by Adam Clark Estes to io9
We’re not saying it’s aliens, but a team of scientists has just discovered a glowing purple orb at the bottom of the ocean, and if you’ve ever seen The Abyss, I think you know how this will end.
by Maddie Stone on Gizmodo, shared by Adam Clark Estes to io9
The smell hit me as soon as I opened my car door—like rancid milk mixed with dog shit. I gasped for breath as humid air descended, filling my pores with the putrid odor.
by Ria Misra on Gizmodo, shared by Adam Clark Estes to io9
The United States wastes over 140 trillion calories of perfectly good food
every year. A national survey just provided a comprehensive overview of the reasons we waste so much—and one of the most common ones is based on a total misconception.
by George Dvorsky on Gizmodo, shared by Adam Clark Estes to io9
Britain is saying goodbye to the European Union, a monumental decision that’s triggering some serious alarm bells among the country’s researchers. Here’s why they have a right to be worried.
San Francisco A.I. startup Anki has a great reputation for making robot cars you can race with your phone. And considering all three founders got their start at Carnegie Mellon’s Robotic Institute
, that’s really no surprise—making little cars you race around a track should be a piece of cake for these guys. But their next trick—an adorable robot called Cozmo—is one of the coolest leaps in toy technology since baby dolls starting soiling their own diapers.
Tip: Remember to shop at children’s stores, too — quite often they have colorful, “less serious” decor that is great for our midcentury modern and midcentury modest homes. Case in point: Thanks to Emily for this great tip about a new Charley Harper collection for Land of Nod. That shower curtain — I LOVE IT!
I was flipping through my deadtree archive of magazines recently when I came across an ad for an ingenious little door alarm in 1906. Granted, it’s not fancy. But it probably did the trick.

























{kind=link}
{kind=link}




 Help is on the way, both in person and online. At ALA Annual 2016, the Copyright Answer booth is back. On Saturday and Sunday only, from 10am – 4pm, conveniently located in the Orange County Convention Center outside of the Exhibit Hall and staffed by copyright librarian experts, stop by and pour your heart out. What copyright issue is troubling you? Feel like venting? We have been there and done that. We will listen, and provide non-legal, but well informed advice.
Help is on the way, both in person and online. At ALA Annual 2016, the Copyright Answer booth is back. On Saturday and Sunday only, from 10am – 4pm, conveniently located in the Orange County Convention Center outside of the Exhibit Hall and staffed by copyright librarian experts, stop by and pour your heart out. What copyright issue is troubling you? Feel like venting? We have been there and done that. We will listen, and provide non-legal, but well informed advice.
















 Tip: Remember to shop at children’s stores, too — quite often they have colorful, “less serious” decor that is great for our midcentury modern and midcentury modest homes. Case in point: Thanks to Emily for this great tip about a new Charley Harper collection for Land of Nod. That shower curtain — I LOVE IT!
Tip: Remember to shop at children’s stores, too — quite often they have colorful, “less serious” decor that is great for our midcentury modern and midcentury modest homes. Case in point: Thanks to Emily for this great tip about a new Charley Harper collection for Land of Nod. That shower curtain — I LOVE IT! The Ladybug quilt comes in Twin and Full/Queen.
The Ladybug quilt comes in Twin and Full/Queen. And ooooh the Flock of Birds rug!
And ooooh the Flock of Birds rug!